Auto logout in seconds.
Continue Logout
What was: Last year’s predictions and what happened
Despite its difficulty, commercial shared savings is seeing renewed interest: Too soon to tell
We predicted increased participation in commercial shared savings in 2025, particularly directed by employers looking for more control over costs. We were right about the industry’s growing appetite for commercial risk agreements.1 According to the 2025 Alternative Payment Model survey, 70% of payers expect alternative payment model (APM) activity to increase over the next 24 months, reinforcing federal and private‑sector commitment to advancing value-based care (VBC). But, with contracting complexity and long implementation timelines, it’s too early to judge recent progress in commercial VBC. As payers and providers adopt strategies for more successful contracting, we expect to see measurable progress that matches industry appetite for advancing commercial shared savings.
All eyes are on Medicare Advantage (MA) as leaders reset their strategy: Mostly correct
We predicted that turbulence within the MA line of business and policy uncertainty would create an inflection point, pushing provider organizations and health plans to either retreat from MA or accelerate and differentiate their involvement.
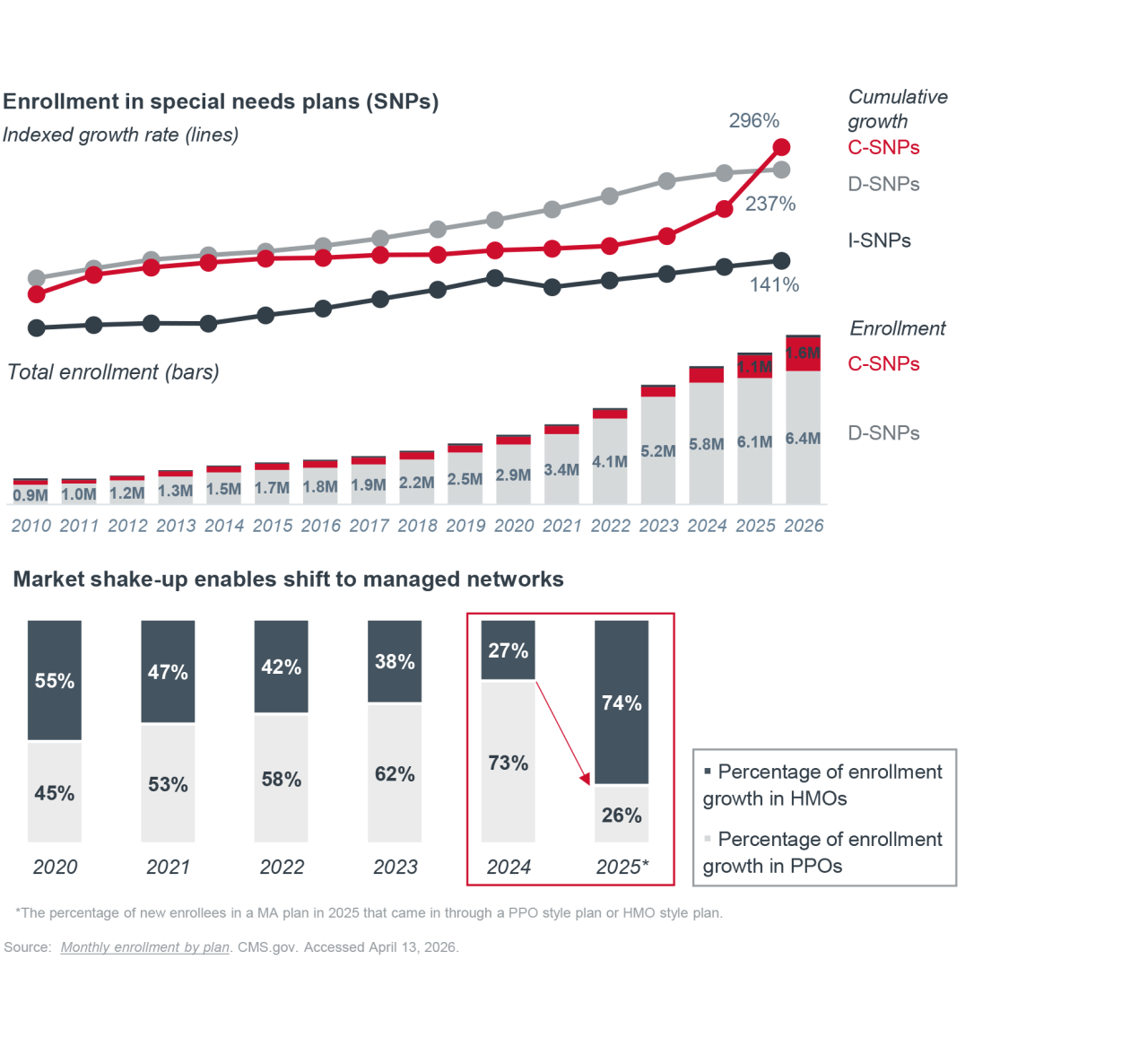
In 2025, multiple provider organizations terminated contracts with certain MA plans, due to administrative burden and reimbursement challenges.2 Additionally, several regional plans,3 multiple Blues plans,4 and large nationals5 announced market exits — citing various financial pressures as their reason for scaling back. As reimbursement lags rising care costs, health plans that remain in the MA market are tightening their playbooks to protect margins. The focus is shifting from rapid enrollment growth to higher‑margin members and stronger management of existing populations. This shift is reflected in the expansion of Special Needs Plans (SNPs), especially Community Special Needs Plans (C-SNPs), and a growing enrollment in Health Maintenance Organization (HMO) plans over Preferred Provider Organization (PPO) plans. Together, these moves signal a push toward more predictable risk and a tighter network.

Value-based care is coming for specialists: Spot on
We predicted specialists were going to start to feel the impact of VBC. We asked, "Is 2025 the year we start to meaningfully engage them in VBC?” The short answer, yes.
Further, we wondered, “how might it look different for different specialties like those that focus more on chronic disease or those that are more procedural in nature?" Finalization of mandatory models like the Transforming Episode Accountability Model (TEAM) and Ambulatory Specialty Model (ASM) demonstrate the Center for Medicare and Medicaid Innovation’s (CMMI) commitment to meaningfully engaging specialists by tying performance to episodes and conditions, rather than volume alone. TEAM encourages care coordination to reduce episode cost variation across high-cost procedures, while ASM creates accountability for specialists to improve chronic disease prevention, early diagnosis, and disease management.
Specialist involvement continues to drive VBC advancement. When asked about what would encourage more investment in VBC, healthcare leaders agree that “policy structures that threaten strategic service line revenue generation” motivate them to act. Both TEAM and ASM do exactly that.
That growing focus on specialists and momentum from CMMI are key themes that we anticipate will continue shaping VBC in 2026.
What’s now: What 2025’s trends mean for VBC today
CMMI is serious about accountability
Compared to previous iterations of CMMI, the current administration was quick to act, creating6 and terminating7 several models during the first year in office. In addition to an increased level of activity from CMMI, there’s been a notable shift in the type of activity and what it means for the future of VBC.
CMMI ended four models early after determining they were unlikely to meet cost savings expectations. New models prioritize accountability, demonstrate recognizable cost savings, and appeal to a broader range of providers (including specialists, those new to Accountable Care Organizations (ACOs), rural-based practices, those caring for high-need populations, and digital health companies). For example, the Advancing Chronic Care with Effective Scalable Solutions (ACCESS) Model introduces outcome-based payments to a wide variety of Medicare Part B–enrolled provider and technology organizations engaged in chronic disease management. The Long-term Enhanced ACO Design (LEAD) Model, replacing ACO REACH at the end of 2026, will have a 10-year downside risk model starting on day one of participation. This is the longest performance period tested to date and will require sustained performance and lower total cost of care, rather than temporary gains.
CMMI has signaled that VBC will remain a priority in 2026, but participation must prove results.
This is a pivotal moment. CMMI is no longer just an innovation lab, it’s becoming a fiscal performance engine. Saving costs is the expectation. The future of VBC will be leaner, faster, and more financially accountable — driven by more mandatory participation and downside risk bearing.

So, are these shifts positive for the future of VBC? Do we know yet?
Historically, healthcare leaders have criticized CMMI for focusing more on experimentation than execution. Some leaders argue that adding more models perpetuates an old habit of reinventing the wheel when the current approach is falling short. While it’s too soon to tell whether current shifts will be positive for the future of VBC, research has long supported the need for more tangible, meaningful downside risk to achieve desired impacts.8 CMMI’s growing emphasis on accountability seems to align with that. As these models take form, we’ll continue to monitor whether they can solve long-standing challenges with VBC execution, or if they are just a new type of experimentation.
"[CMMI’s strategic] pillars are underpinned by a foundational principle, which is to protect the federal taxpayer… The Innovation Center will focus on models that show the greatest promise for generating savings and improving quality."
Abe Sutton
Director of CMMI
What’s next: In 2026, we face 2 existential questions about the future of VBC
How does the One Big Beautiful Bill Act (OBBBA) impact the future of VBC?
Beyond changes from CMMI, broader volatility in the healthcare industry has left leaders questioning where VBC fits into this new reality.
The OBBBA shook up the healthcare industry in 2025. Because of the general uncertainty for what’s to come, there’s an assumption that leaders might err on the side of risk avoidance and pull back from VBC initiatives. Though, based on our conversations in the market, the opposite seems to be true. At our 2025 VBC Roundtable we asked 50 healthcare executives, “Is OBBBA going to accelerate, deter, or have no impact on VBC?” All but one person said that they were increasing their VBC efforts despite the shifting environment.
While it's too soon to fully understand the long-term impact, history suggests that periods of disruption can make VBC more attractive. During COVID-19, VBC offered more consistent revenue despite changes in volume. What we do know is, with rising labor costs, persistent inflation, and shifts in reimbursement pressure, many organizations are continuing to view VBC as a strategic pathway to stability and long-term growth.
How will VBC account for the growing role of therapeutic drugs?
Therapeutic drugs are becoming increasingly central to modern care. Rising use of specialty drugs, biologics, gene therapies, and high‑cost chronic treatments is now a major driver of healthcare costs.9 However, they remain largely carved out of VBC contracts due to the complexity of tracking long-term outcomes.10 Still, policy efforts continue to prioritize drug prices. CMMI’s new drug payment models and site neutral payment policies focus on reducing the upfront costs associated with procuring and delivering medications. Though, we've yet to see widespread adoption of outcome-based risk-sharing models for therapeutic drugs. As a result, one of the fastest-growing cost drivers in healthcare remains only partially integrated into VBC.
Final thoughts
Despite feelings of turmoil in 2026 and naysayers claiming that “VBC is so yesterday”, VBC is still here to stay — and it’s taken on a new flavor. Healthcare leaders report accelerating or recommitting to their VBC efforts in more deliberate and sustained ways. In this next era of VBC, healthcare leaders must learn to adapt to — and embrace — additional risk and cross-industry collaboration. The future success of VBC will depend on deeper engagement from specialists, technology companies, and pharmaceutical partners. Organizations that will win are the ones that find new ways to work with industry partners to evolve their VBC strategy.
1 Driving commercial value‑based care adoption. Health Care Transformation Task Force. June 30, 2025.
2 Emerson J. 16 health systems dropping Medicare Advantage plans in 2026. Becker’s Hospital Review. December 30, 2025.
3 Stefanescu V. UCare terminates Medicare Advantage plans for 2026 amid financial turmoil. Star Tribune. September 4, 2025.
4 Vermont Blue Advantage leaves Medicare Advantage market. Vermont Department of Financial Regulation. October 1, 2025.
5 Pifer Parduhn R. UnitedHealthcare, Humana, Aetna scale back Medicare Advantage plans for 2026. Healthcare Dive. Published October 2, 2025. . January 10, 2026.
6 Innovation Center models. CMS. March 16, 2026.
7 CMS Innovation Center announces model portfolio changes to better protect taxpayers and help Americans live healthier lives. CMS. March 12, 2025.
8 Richard Jackson, Kevin Dotson, Munzoor Shaikh. The key role of downside risk in the success of value‑based care. HFMA. June 5, 2024.
9 Key drivers of 2026 health care cost increases. NIS. Accessed April 13, 2026.
10 Laurent A. Value‑based contracting in pharmaceuticals: models and challenges. IntuitionLabs. February 23, 2026.




Posted on April 15, 2026
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox