Auto logout in seconds.
Continue Logout
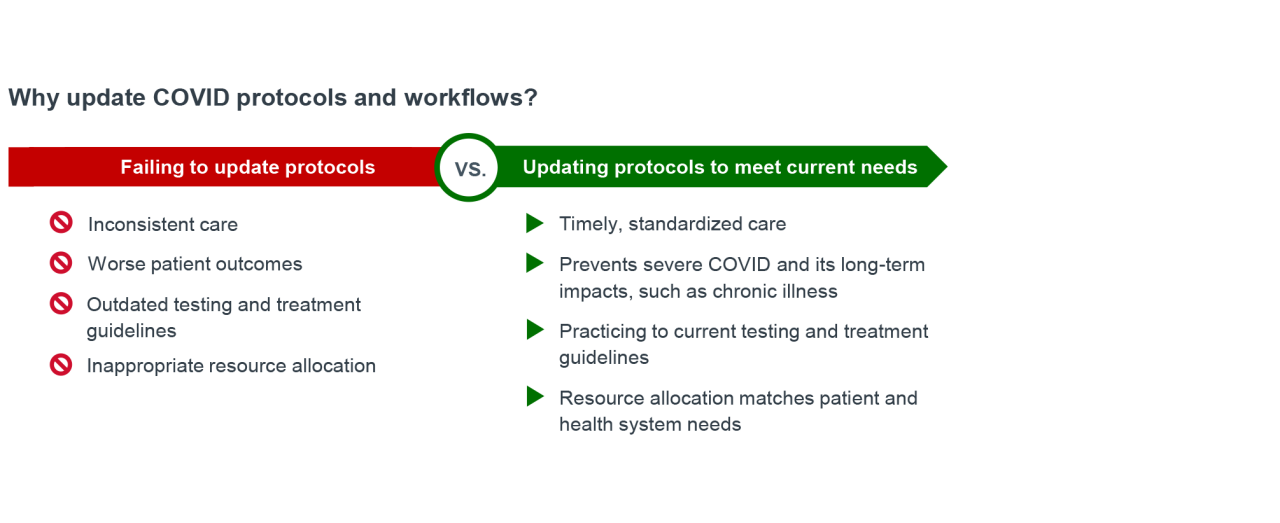
Why updating COVID-19 protocols is necessary
Researchers and clinicians are still learning about the impacts of COVID on patient health.1 For instance, the illness can start or worsen chronic conditions like asthma,2 heart disease,3,4 or diabetes.5,6 COVID-related chronic illness may also worsen patient outcomes, resulting in additional strain on the healthcare system.7 Healthcare leaders must continue to manage COVID as a common, year-round respiratory illness with the potential for long-term impacts.
During the pandemic, many health systems rapidly developed COVID workflows and patient pathways to respond to the emergency.8,9,10 Those protocols were often designed to allocate resources and prioritize patients with the most severe illness to receive emergent treatments. Some of these ad hoc workflows were resource and labor intensive, making them unsustainable long-term, but other approaches may continue to help optimize today’s COVID care. For example, the same clinical informatics tools health systems used to enhance workflows during the emergency — including enhanced clinical decision support (CDS), telehealth capabilities, and streamlined communication and documentation11 — can support health systems as they navigate COVID’s endemic era.
Hospitals and health systems have an opportunity to update their workflows to prevent severe COVID and its long-term impacts by:
- Incorporating and continually updating guideline-endorsed COVID testing and treatment options in outpatient and acute care settings.
- Using standardized, streamlined workflows that prioritize timely testing and treatment, preserving resources.
Updating care standards could help providers deliver appropriate COVID treatment and enhance performance on quality metrics. According to the Centers for Disease Control and Prevention (CDC), when COVID medicine is taken early it can help stop serious illness,12 which can lower the risk of new or worsening chronic conditions.2-6
How to standardize COVID protocols in the electronic health record
Leverage CDS for consistent diagnosis and treatment
Providers may not always be current on every aspect of COVID care, such as risk factors for severe illness, drug-drug interactions (DDIs), product label updates including severe renal impairment (SRI), or reputable testing and treatment guidelines. Without a standardized screening and treatment process, providers may miss less visible risk factors, such as being unvaccinated or having an underlying condition,13,14 and some patients may not get appropriate care. For instance, when those risk factors are overlooked, a provider’s decision to prescribe an antiviral could hinge on the provider’s opinion or a patient’s request, rather than patient eligibility or standards of care.
To help providers make consistent treatment decisions, health systems can leverage CDS tools in the electronic health record (EHR) to deliver a standardized COVID protocol. In addition to reminding providers to consider the risk factors and the potential for long-term illness, these tools can direct them to current testing and treatment guidance.
"There's no built-in decision tool in our EHR for who should and shouldn't get treatment, so it is very inconsistent. I think that's a problem."
Clinical research director and physician, emergency medicine
Nonprofit academic medical center
A range of EHR-capable CDS tools can help providers capture and treat more patients at risk of severe COVID:
- CDS alerts (i.e., the Epic® OurPractice Advisory functionality) appear in the clinician’s workflow. Alerts suggest actions like entering orders, opening documentation tools, or simply acknowledging the alert.
- CDS pathways (i.e., pathway tools such as AgileMD®) integrate evidence-based decision support within the EHR to help clinicians make care decisions with step-by-step recommendations, suggested orders, and documentation prompts.
Risk factors and treatment protocols often included in the EHR
| Screening and diagnosis |
|
|---|---|
| Treatment decisions |
|
| General education |
|
*Black, indigenous, and people of color. | |
Incorporate data collection into COVID workflows to track and improve quality measures
Many health systems already track some of the conditions that worsen or develop because of COVID, but not the relationship between the illness and those conditions. But there is a connection: Because severe COVID can lead to new or worsening chronic conditions,2-6 lowering rates could improve related quality measures.
By implementing a standardized process for data collection in the EHR, health systems extract the baseline data needed to begin evaluating patient outcomes in relation to COVID. Specifically, the quality management team can run reports to see the correlation among COVID severity, intervention, and related chronic conditions.

*See endnote 15.
How to streamline workflows and reduce burden
Use EHR tools to streamline documentation
In addition to enabling consistent care, standardized protocols should be designed to save time for clinicians. In high-volume, acute care settings like the emergency department or urgent care, providers have limited time with each patient. There are opportunities to create more streamlined workflows that put information all in one place and reduce the burden of documentation.
Health systems can use a range of EHR capabilities to streamline the documentation process for providers evaluating patients with symptoms of COVID:
- Dot phrases (i.e., Epic® SmartPhrases) are shortcuts that trigger a block of text when a provider types a key word or phrase in the EHR, inserting frequently used phrases or instructions. By inserting predefined, structured text into documentation, dot phrases allow clinicians to capture the same essential documentation elements and can include templated patient instructions.
- Guideline-based treatment tools (i.e., Epic® SmartSet or Express Lane) bundle together orders, diagnoses, documentation templates, and patient instructions.
"You want to reduce the burden of thinking about documentation as much as possible, so I have a dot phrase that walks me through it."
Clinical research director and physician, emergency medicine
Nonprofit academic medical center
As COVID research evolves and care guidelines are updated, shortcuts and templates can help health systems ensure all providers have the most current guidance in one place by updating the EHR directly. Health systems that have implemented these functions indicate improved consistency across documentation and increased provider satisfaction with a less burdensome process.
Leverage alternative care team members to prevent gaps in care
In addition to leaning on EHR tools to create a more streamlined workflow, there is an opportunity to create workflows that leverage additional care team members.
For example, when treating COVID, providers need a full understanding of a patient’s current medication list to avoid a potential DDI between an existing medication and prescribed COVID treatment. But some settings, such as emergency departments (EDs) or acute care clinics, may not have access to patients’ complete health records, and providers may not have time to collect a full history of present illness (HPI) or do a medication reconciliation (MedRec) during a short visit for respiratory symptoms.
To address this, one health system has stationed pharmacists in the ED to manage the MedRec process for admitted COVID patients with specific comorbidities, such as asthma, congestive heart failure, hypertension, or diabetes.
First, a pharmacist can be notified when a patient is admitted to the ED with comorbidities involving medications that may interact with common COVID treatments. The pharmacist then conducts a detailed MedRec to understand the patient’s current medication list and collect information to ensure treatment decisions are safe and medications for chronic illness are maintained after COVID treatment.
Pharmacists also deliver medications to the patient directly, educate them about prescriptions, and answer questions. In this way, health system pharmacists play a key role in preventing inconsistencies in COVID care, save time for physicians, and create positive patient experiences — as reflected through their Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) and Press Ganey scores.
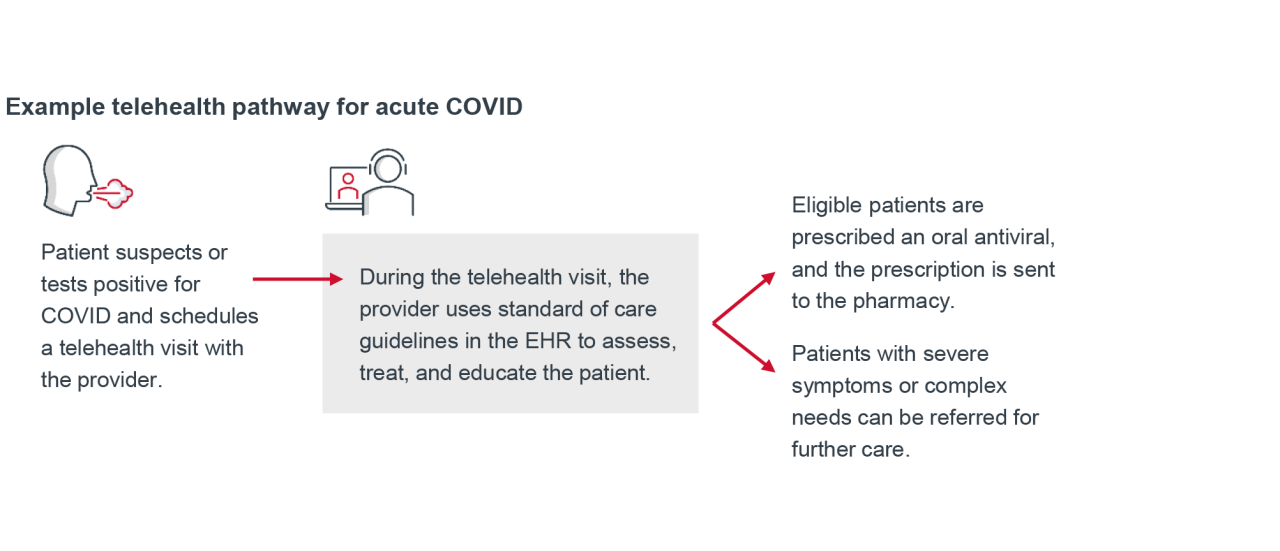
Use telehealth for timely COVID evaluation and treatment
During the pandemic, telehealth visits reached an all-time high. Today, telehealth remains a valuable tool for delivering comprehensive and timely COVID care. Some health systems use telehealth to evaluate patients who suspect they have COVID or have tested positive. After evaluating the patient’s symptoms, risk level, and potential DDIs, providers may prescribe an oral antiviral, offer supportive care options, or refer the patient to in-person care. Also, if a patient receives a COVID test result after leaving an in-person appointment, providers can use telehealth to follow up with information about patient eligibility, DDIs, and next steps.
By assessing patients quickly through telehealth, providers can treat patients within a few days of symptom onset — a critical window for preventing progression to severe COVID. In addition, the ED, urgent care, and on-site primary care settings may see reduced volumes, shortened patient wait times, and a lower risk of COVID transmission.
Amplify impact by combining pharmacist and telehealth strategies
A pharmacist-driven telehealth service expanded timely access to COVID oral antiviral medications, especially for older, high‑risk patients. By assessing patients and prescribing medications through telehealth, the service overcame common challenges to timely treatment, including physician shortages, high patient volumes, geographic barriers, and risk of complex drug interactions. In doing so, the telehealth service more easily navigated complex treatment criteria and drug interactions, ultimately reducing treatment delays.16
1 day
Median time from symptom onset to antiviral prescription, using pharmacist-driven telehealth
Final thoughts
COVID continues to have immediate and long-term effects on patient health and health system operations. Emerging research shows that the virus can trigger or worsen chronic conditions. As knowledge evolves, health systems must establish standards of care for consistent diagnosis and timely treatment to help improve patient outcomes and reduce added strain on the healthcare system.
Updating workflows to address these long-term impacts may encourage sustainable, standardized care and improve patient outcomes and quality metrics.
Taking stock of your organization’s current approach to COVID care will help identify a strategy that meets the needs of patients, clinicians, and staff. Review your current COVID protocols by asking yourself the following questions:
- Which pandemic-era protocols do we no longer use due to time and/or resource constraints?
- Which protocols could be updated for today’s COVID care? Updates to those protocols may include high-risk factor identification, testing, treatment with an oral or IV option, DDI management tools, and FDA label updates indicating expanded populations.
- Do clinicians have the tools they need to efficiently assess patient risk level? If not, how can we provide those tools?
- Are there risk factors for severe COVID that are often overlooked? Which ones?
- Do clinicians have updated guidelines to confidently test and prescribe treatment for COVID? How is that guidance updated?
- Which COVID processes place undue burden on clinicians?
- How might we leverage pharmacists or other members of the care team to effectively provide COVID care?
- Is the organization effectively using telehealth to expand patient access to care?
1 Unless otherwise noted, all information in this case study came from Advisory Board interviews with officials from four health systems. Brand name EHR tools mentioned in this document were used at one or more of these health systems.
2 Kim B, et al. Increased Risk of New-Onset Asthma After COVID-19: A Nationwide Population-Based Cohort Study. J Allergy Clin Immunol Pract. September 27, 2023.
3 Zuin M, et al. Risk of incident heart failure after COVID-19 recovery: a systematic review and meta-analysis. Heart Fail Rev. December 27, 2022.
4 Hilser JR, et al. COVID-19 is a coronary artery disease risk equivalent and exhibits a genetic interaction with ABO blood type. Arterioscler Thromb Vasc Biol. October 9, 2024.
5 Mehrotra-Varma S, et al. Patients with type 1 diabetes are at elevated risk of developing new hypertension, chronic kidney disease and diabetic ketoacidosis after COVID-19: Up to 40 months' follow-up. Diabetes Obes Metab. September 2, 2024.
6 Xie Y, Al-Aly Z. Risks and burdens of incident diabetes in long COVID: a cohort study. Lancet Diabetes Endocrinol. March 21, 2022.
7 Pike J, et al. Direct Medical Costs Associated With Post–COVID-19 Conditions Among Privately Insured Children and Adults. Preventing Chronic Disease. February 9, 2023.
8 Wendel SE, et al. Successful Implementation of Workflow-Embedded Clinical Pathways During the COVID 19 Pandemic. Quality Management in Health Care. July/September 2023.
9 Hinson JS, et al. Multisite implementation of a workflow-integrated machine learning system to optimize COVID-19 hospital admission decisions. Nature. July 16, 2022.
10 Vilendrer S, et al. Nursing Workflow Change in a COVID-19 Inpatient Unit Following the Deployment of Inpatient Telehealth: Observational Study Using a Real-Time Locating System. J Med Internet Res. June 17, 2022.
11 Hsu H, et al. Clinical informatics during the COVID-19 pandemic: Lessons learned and implications for emergency department and inpatient operations. J Am Med Informatics Assoc. November 28, 2020.
12 Types of COVID-19 Treatment. Centers for Disease Control and Prevention. February 6, 2026.
13 Underlying conditions include heart disease, diabetes mellitus, chronic lung disease, chronic kidney disease, brain or nervous system diseases, chronic liver disease, unmanaged HIV, mood disorders or schizophrenia, dementia, having received an organ or stem cell transplant, sickle cell anemia and thalassemia blood disorders.
14 Mayo Clinic Staff. COVID-19: Who's at higher risk of serious symptoms? Mayo Clinic. Accessed December 5, 2025.
15 Measure inventory. Centers for Medicare & Medicaid Services. Accessed September 10, 2025.
16 Potter J, et al. Impact of a pharmacist-led collaborative approach to care for treatment of COVID-19 in the outpatient setting. Am J Health-Syst Pharm. April 1, 2025.
A note about this research
This document was developed to illustrate several healthcare organizations’ experiences with updating COVID protocols. Pfizer did not provide direct financial support for the work completed. Participants from the health systems interviewed were compensated for their time in providing these insights.
All development and implementation, including HIT functionality, were solely chosen, implemented, and maintained by these health systems. Pfizer does not endorse or recommend any specific functionality discussed within this resource. Each health system is solely responsible for determining which EHR functionality to implement and for implementation of such functionality. All treatment decisions must be decided by the healthcare professional in consultation with the patient after review of the patient’s full medical history.
This resource was not reviewed or endorsed by Epic® or AgileMD®. All trademarks are the property of their respective owners. Pfizer does not guarantee any outcomes if health systems choose to implement similar initiatives.
At Pfizer, we’re in relentless pursuit of breakthroughs that change patients’ lives. We innovate every day to make the world a healthier place. Our unique resources allow us to do more for people. Using our global presence and scale, we’re able to make a difference in local communities and the world around us.
Pfizer supports the global healthcare community’s independent quality improvement initiatives to improve patient outcomes in areas of unmet medical need that are aligned with Pfizer’s medical and/or scientific strategies. For more information, please visit www.pfizer.com.
This report is sponsored by Pfizer, an Advisory Board member organization. Representatives of Pfizer helped select the topics and issues addressed. Advisory Board experts wrote the report, maintained final editorial approval, and conducted the underlying research independently and objectively. Advisory Board does not endorse any company, organization, product, or brand mentioned herein.
To learn more, view our editorial guidelines.
This report is sponsored by Pfizer. Advisory Board experts conducted the underlying research independently and objectively.

Jennifer Fierke
Senior writer and editor, Sponsorship
Posted on April 01, 2026
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox