Auto logout in seconds.
Continue LogoutEditor's note: This popular story from the Daily Briefing's archives was republished on Jan. 3, 2020.
Read Advisory Board's take: The term we use in our research
An overwhelming majority of physician assistants (PAs) believe there is a disconnect between their job title and what they actually do, according to new research from research firm WPP, amplifying the debate about whether a title change may be in order.
A disconnect
WPP's research was initiated a year ago by the American Academy of PAs' (AAPA) House of Delegate's Title Change Investigation. The goal was to investigate how feasible changing the legal title of the PA profession might be.
For the research, WPP surveyed almost 6,000 PAs and 1,300 PA students, and conducted a second study focusing on qualitative interviews and focus groups of more than 50 people.
The researchers found 90% of PAs said there was a disconnect between their title and their role in health care.
The research suggests that PAs are viewed favorably across all stakeholder groups, but that the title "physician assistant" was not congruent with the PA's roles or responsibilities. Namely, the researchers found most PAs believe the role "assistant" does not accurately describe what PAs are able to do, and could cause confusion among patients.
WPP is currently doing more quantitative research with physicians, employers, and patients.
Comments
The findings drew interest from several PAs on LinkedIn.
For example, Laura Record-Halpern, a PA at Providence Medical, said that she has "a license to practice medicine and a DEA license just like the [physicians] do." Because of that, and her role within the hospital, she said "we are no one's 'Assistant'.' She continued, "We are an associate, an extender, but not an assistant. There is no handholding here after years of experience … We do not practice as assistants and the patients still DO NOT GET IT. It is exhausting explaining to them our scope of practice, expertise, and that we perform the same exact tasks (depending on the practice) as the physicians do." She added, "We are clinicians. Period."
Kooper Underwood, a PA student, suggested changing the name to either "medical practitioner" or "physician associate."
Similarly, Rosalyn Rosas, a PA at Oxford University Hospitals NHS Foundation Trust, said, "I strongly believe that Physician Associate is the appropriate title for the profession. … We have to work together to improve and protect our profession to avoid confusion."
However, not everyone supports changing the name. Kristina Brown, a PA and quality manager at SUNY Downstate Medical Center, said she thinks the title should stay as is. "We are dependent practitioners at the end of the day," she said. "I rely on a [p]hysician to hire me, supervise me, teach me, consult with me, and collaborate with me. I cannot start a practice on my own. I also did not attend school or training nearly as long or leave school with the same tuition bill … I don't have the same responsibility as them or liability and I like it that way!"
Similarly, Scott Tatum, a cardiothoracic surgery PA, said the current title "is just fine." He added, "The respect from patients comes from the way you care for them, not your name or title."
Taylor Campbell, a PA at US Acute Care Solutions, said, "I can't buy into the whole patient confusion argument," and argued that changing the word from "assistant" to "associate" wouldn't change anything. "I can hear patients still asking, 'what's a physician associate?' [S]ame conversation. Different name," Campbell said (AAPA press release, 5/19; Kutscher, LinkedIn, 5/23).
Advisory Board's take


Julie Riley, Practice Manager, Physician Practice Roundtable; andSarah Hostetter, Consultant, Physician Practice Roundtable
As this study shows us, titles can have tremendous power—particularly in the health care field where expertise and trust are so important. This is probably why we are often asked by members: What should nurse practitioners (NPs) and physician assistants (PAs) be called in our medical practice?
We know that NPs and PAs are increasingly taking on more autonomous roles in practices. Although they're often taking on a provider role, they are not doctors by training. This creates a dilemma: While we can't call them doctors, many of the alternative terms that are often used can belittle the essential contributions they make to expanding access, improving quality, and offsetting physician workloads.
For instance, terms like 'mid-level provider' and 'physician extender' reflect an outdated understanding of the role these practitioners actually play in care delivery. More specifically:
- 'Mid-level provider' suggests that they have either a lower hierarchical standing (relative to 'high-level' physicians) or offer lower quality care. But our research has shown that across the country, these practitioners are assuming greater autonomy and taking on their own panels, while evidence demonstrates that APPs offer care of comparable quality to that of physicians; and
- The term 'physician extender' is even less applicable, since it fails to capture the provider-level work that APPs frequently perform. Indeed, where medical groups use APPs to just "extend" the physician, they likely are underutilizing their APPs, and could task RNs, LPNs, or others with those assistant duties.
While this nomenclature may seem inconsequential, we know that names have power—both over the existing culture and the culture that your practice wants to build. Our research suggests that medical groups that use their APPs most extensively and effectively also bestow titles commensurate to their role and value. Indeed, groups that are working toward deploying APPs consistently at top-of-license consider a change in terminology as part of their broader effort.
In our research, we use the term 'advanced practice provider' (APP), though some organizations prefer 'advanced practice clinicians' or other variants on the theme. This helps convey the value of APPs and highlights their role within the organization—to themselves, their care teams, and patients.
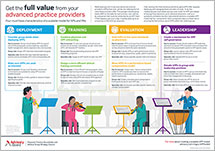
Want to learn more about how to make the most of your advanced practice providers? Download our new infographic which outlines four components of a scalable model for APPs.
Then, if you're a Physician Practice Roundtable or Medical Group Strategy Council member, view our toolkit to access additional resources to help you develop a high-value, scalable, APP model.
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox