Auto logout in seconds.
Continue LogoutPatients often detail their care preferences and end-of-life decisions in documents such as living wills and "do not resuscitate" (DNR) orders, but research suggests providers often misunderstand these documents—and may violate patients' wishes as a result, Judith Graham reports for the Washington Post.
Advance a shared definition for inpatient palliative care
What happens when providers misinterpret end-of-life decisions
According to Graham, few health systems and state regulators treat end-of-life document misinterpretations as medical errors that must be tracked and reported. But data from some states, such as Pennsylvania, offer a glimpse at the prevalence of misinterpretations.
For instance, a recent report found Pennsylvania-based health care facilities in 2016 reported nearly 100 events related to a patient's "code status," or their desire to be resuscitated. Of those 100 events, 29 patients were resuscitated against their wishes, while two patients were not resuscitated despite stating in their documents they wanted to be resuscitated. The remaining 69 cases were described as "near misses."
According to Regina Hoffman, the executive director of the Pennsylvania Patient Safety Authority, a near miss could involve a physician who assumes a DNR applies to a patient who develops a serious infection after an elective surgery but whose error is corrected by a colleague.
Ferdinando Mirarchi, the medical director of emergency medicine at the University of Pittsburgh Medical Center Hamot in Pennsylvania, has explored the topic through surveys posing hypothetical scenarios. For instance, in one survey physicians were asked how they would respond if a 46-year-old woman—who's otherwise healthy and has a living will—presented at the ED with a heart attack and quickly goes into cardiac arrest.
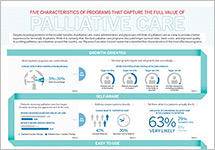
Just 43% of the more than 700 surveyed doctors said they would intervene to save the patient's life. Mirarchi said this number is concerning since the hypothetical patient had no terminal condition and, as a result, her living will would not apply.
In one real-life instance, a nurse told Monica Williams-Murphy, medical director of advance-care planning and end-of-life education for Huntsville Hospital Health System, "Don't resuscitate this patient. He has a living will." But when Williams-Murphy actually read the patient's document, she discovered that he in fact wanted all possible treatment, including CPR.
Williams-Murphy acted quickly and revived the patient, who eventually recovered.
Why providers are at risk of misunderstanding end-of-life wishes
The source of the confusion, according to Hoffman, is a lack of training. Doctors generally receive little training—if any at all—on how to understand and interpret DNR orders, living wills, or Physician Orders for Life-Sustaining Treatment (POLST) forms, Graham reports. That lack of training, Graham writes, is further compounded by the speed at which these life-and-death decisions often must be made.
But Arthur Derse, director of the center for bioethics and medical humanities at the Medical College of Wisconsin, cautions that occasional misinterpretations should not discourage patients from having a medical directives. "Are there errors of misunderstanding or miscommunication? Yes. But you're more likely to have your wishes followed with one of these documents than without one," he said.
The differences between end-of-life forms
Understanding the difference between various end-of-life documents is important for both patients and physicians, Graham reports.
Living wills: A living will is not "a binding medical order," and it does not apply until one or two physicians agree that the patient is "terminally ill and unconscious or in a permanent vegetative state," Graham writes. It allows the patient to state end-of-life preferences for medical staff to follow and interpret with the patient's family or surrogate decision-maker. For instance, living wills can state that a patient does not want cardiopulmonary resuscitation (CPR) if he or she stops breathing.
DNRs: DNRs "are binding medical orders, signed by a physician," Graham writes. But they apply only to cardiopulmonary resuscitation (CPR), instructing medical staff not to administer chest compressions "if someone stops breathing or their heart stops beating." A DNR does not necessarily mean a patient has refused other forms of medical care, such as mechanical ventilation or intubation.
POLST forms. A POLST form is another type of medical order signed by a physician, physician assistant, or nurse practitioner, but unlike DNRs, they are specifically intended for patients expected to die within a year. The forms can vary by state, according to Graham, but they are intended to be created after "detailed conversation about a patient's prognosis, goals and values, and the potential benefits and harms of various treatment options." Amy Vandenbroucke, executive director of the National POLST Paradigm, said that POLST forms are "still relatively new" and that "there's education that needs to be done."
Ultimately, Derse said, it's best for patients to make end-of-life decisions with their physicians, a surrogate decision-maker, and their families, especially as their health status changes. Without having that kind of conversation, end-of-life documents can be difficult for physicians to interpret (Graham, Washington Post, 6/14).
How to set the right parameters for your inpatient palliative care program’s goals
This primer examines how four health systems advanced a shared definition for inpatient palliative care and how your organization can set the right parameters for your program's goals.
Download the Primer
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox