Auto logout in seconds.
Continue LogoutOverview
The challenge
Social determinants of health (SDOH) have a major impact on people’s lives, including their well-being and quality of life—and differences in these factors across communities can contribute to wide health disparities. High poverty rates and inequitable distribution of resources in the Rio Grande Valley of Texas drew the attention of CareAllies and their independent physician association (IPA) client in the area—Valley Organized Physicians (VOP).
The organization
CareAllies, a subsidiary of Cigna, supports 66 provider organizations (over 455,000 lives) to help simplify and accelerate growth in value-based care with solutions that help engage providers; optimize value-based contracts with multiple payers; and improve performance, efficiency and patient care. Working with VOP, an IPA located in the Rio Grande Valley in South Texas, CareAllies launched a pilot to better connect VOP’s patients to social resources in their community.
The approach
To help identify VOP patients’ social needs and connect them to appropriate educational resources and community-based organizations (CBOs), VOP and CareAllies launched an SDOH pilot program. CareAllies created a Health Advocate Team – an interdisciplinary team that includes social workers, nurses, and a registered dietician who limit the burden placed on practices by addressing needs in the patient population on behalf of the patient’s primary care physician.
The result
In 2020, more than 1,300 social needs (e.g. food access, financial assistance, transportation needs) were identified by the team. Multiple attempts were made to connect with patients, allowing the team to engage with 85% of the patients. The Health Advocate Team was able to address 97% of identified SDOH needs. The team continues to raise awareness around SDOH and build relationships in the community to increase engagement while identifying more resources to make a difference in the lives of VOP patients.
How CareAllies Approaches SDOH
CareAllies recognized that in the Rio Grande Valley community, the most immediate problem in addressing SDOH needs wasn’t the lack of relevant social resources, but the ability to link patients with organizations and partners they would trust. Despite the availability of certain resources, it was clear that managing all of these connections would be an enormous burden to place on providers and practices alone.
CareAllies’ SDOH partnership with VOP is successful for three main reasons. First, they utilize data and dedicated SDOH resources to support practices, avoiding additional burden. Second, the interdisciplinary team of Health Advocates has expertise, local knowledge and works closely with providers allowing them to identify and address SDOH needs in the best way possible. Third, the team follows through to close the loop and continuously reassesses processes to improve the program.
CareAllies and VOP designed a pilot program to use data and analytics for proactive outreach to patients believed to have unaddressed social needs, while simultaneously fielding referrals from physicians. The pilot, now a fully-implemented program, focuses on key SDOH areas to bridge the gap between patients and relevant resources and relies on CBOs and other partners to maximize access. Key areas include: food access, housing, financial assistance, social support, health education, psychosocial needs, and transportation.
The first step of a successful SDOH support program is to identify who in the population needs support—which can be more challenging than anticipated. CareAllies’ program finds VOP patients with SDOH issues by utilizing multiple sources of data and engaging in conversations at the point of care. Data and analytics are used for proactive outreach within VOP’s patient population, and physician-patient conversations lead to additional program referrals, which is an improved version of many common SDOH programs.
Referral-driven outreach
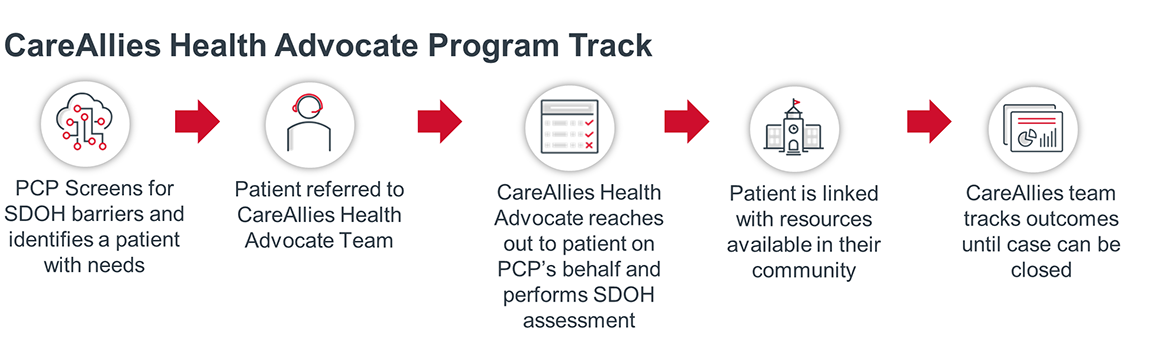
The CareAllies team fields referrals from internal sources like case managers, pharmacists, and medical directors, as well as external sources, like a patient’s PCP, who is seen as a key referral channel. CareAllies encourages VOP’s clinicians to utilize screening tools (like PRAPARE) to identify SDOH needs and to inform patients of the CareAllies outreach. While patients may be suspicious of “out of the blue” outreach, they are more likely to accept help if their trusted PCP informs them of the call beforehand. This is a central concept to CareAllies’ program: build on trust where it already exists.
Once a PCP screens a patient, they can use referral tools from CareAllies to connect the patient to the Health Advocate Team. Once the patient has been referred into the program, a CareAllies Health Advocate contacts the patient to perform a teleassessment designed to identify additional barriers and score patients based on SDOH needs and risk. The assessment helps the program’s staff better triage patients and link them to the appropriate interventions.
Proactive outreach
CareAllies also developed a proactive outreach system for patients with needs that aren’t detected through interactions with clinicians that identifies who might need help overcoming their SDOH barriers.
The CareAllies Health Advocate Team developed this proactive outreach approach for several reasons. For PCPs, conversations about social needs can be difficult, taboo, or time-consuming, which makes it challenging to identify all patients with SDOH-related needs. In addition, patients may be hesitant to speak to their PCP about their needs or may not go to the PCP’s office at all; hence, many issues may go undetected.
In order to conduct this proactive outreach, CareAllies created a Whole Person Health Score algorithm used to prioritize patient outreach and predict success.
The scoring algorithm is based on three main data sets: geographic information, individual data and future cost considerations. Not surprisingly, financial and economic factors play a significant role in the algorithm.
An analytics team is equipped to monitor data flows and identify appropriate outreach targets. This team identifies patients with predicted SDOH needs and stratifies these patients by their overall whole person health risk.
After identifying patients with social needs, the CareAllies team helps resolve their needs by educating them, sharing resources, and referring them to community resources.
The program is operated by the Health Advocate Team, an interdisciplinary team of social workers, registered nurses, dieticians, licensed practical nurses, health equity consultants, pharmacists, and data and analytics experts. The program’s staff stresses cultural competency. Crucially, staff is hired from the community and many speak Spanish to accommodate nearly 90% of the population that identifies as Hispanic in Hidalgo and Cameron counties.
The teleassessment performed when patients are referred into the program mirrors existent screening tools like PRAPARE and helps glean more information for CareAllies and VOP to improve patient outcomes.
There is no “typical” case in terms of length or intervention, given that every patient has a unique set of needs that will need to be addressed. Generally, once the Health Advocate Team reaches out to a patient, connects the patient to a CBO or other resource, and confirms they’ve addressed the root problem of a patient’s SDOH issue – the case is closed. Should new SDOH needs arise in a patient who’s already gone through the program, a new case will be opened.
The program focuses on linking VOP patients with local resources in seven categories: food access, housing, financial assistance, social support, health education, transportation, and psychosocial needs.
A real case example gives greater understanding of how the CareAllies interdisciplinary team works in action.
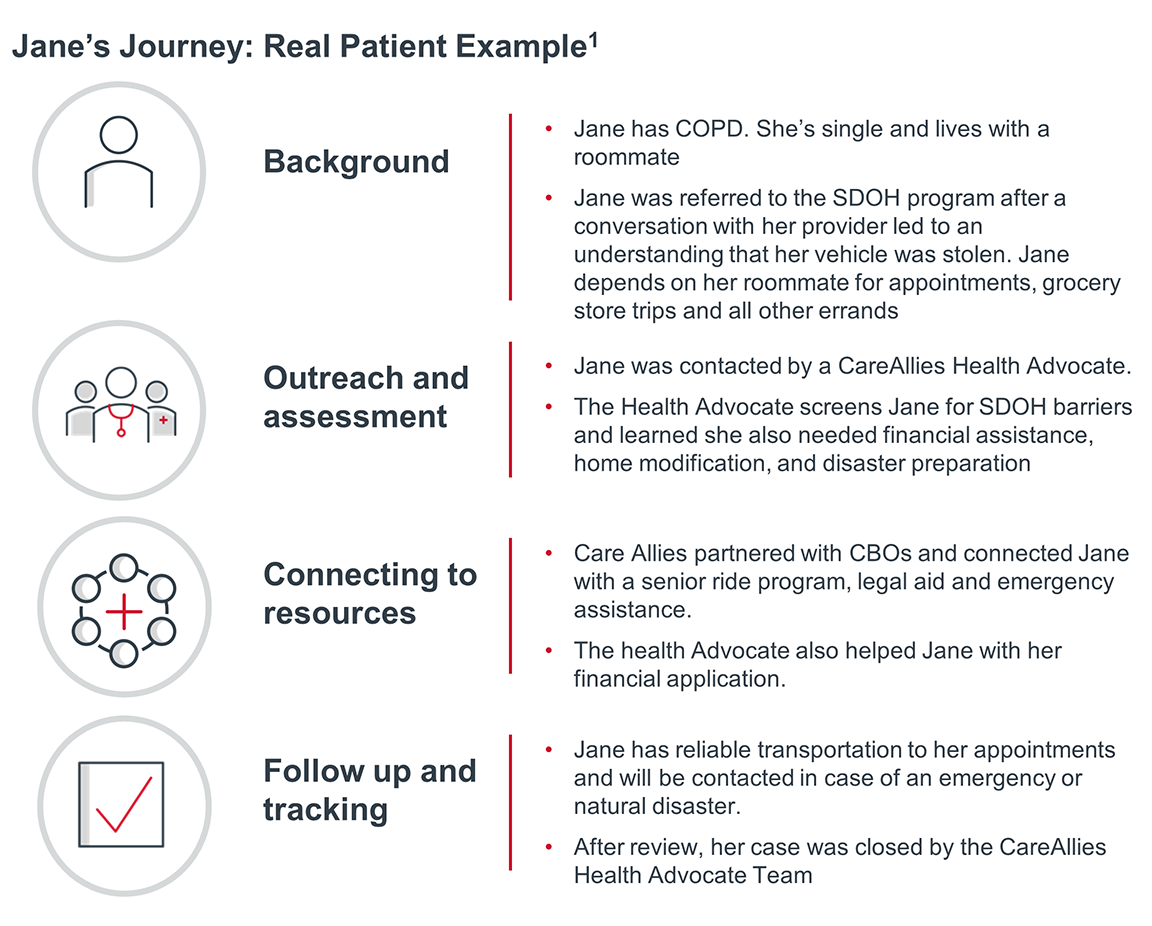
Jane’s PCP was able to identify a barrier that could have been overlooked by data and analytics without considering the human perspective. In addition, CareAllies’ interdisciplinary staff experts were able to dig deeper, identifying additional barriers. By working together, utilizing both data and the physician-patient relationship, the SDOH program has a more significant impact on health outcomes for VOP patients.
CareAllies closely tracks patient outcomes and coordinates follow-up care with the patient’s PCP. The goal of the program isn’t just to connect patients with resources, but to also monitor the whole health of a patient and ensure referred resources are utilized properly.
CareAllies gathers a myriad of data points throughout the care journey to optimize outreach and treatment of those patients in need, and then ensure those needs are being met. For example, the program carefully tracks the length of various processes throughout a patient’s care journey, from the identification of a need, to successful utilization of resources. This information is used by CareAllies to help identify trends and learn what works and what doesn’t, while establishing stronger relationships to better meet the needs of patients.
How we know it’s working
In 2020 CareAllies identitied more than 1,300 SDOH needs across VOP patients. The team was able to engage with 85% of the patients they reached out to and met 97% of the social needs of patients who were eligible and willing to participate.
Early analysis of 2021 data showed fewer identified needs and lower engagement than the previous year; however, 98% of the needs were met for patients eligible and willing to participate. This raises the question – how should the success of an SDOH program be measured, and what can be learned by digging deeper?
- Does a reduction in identified needs mean the program is working?
- Does lower engagement indicate an increase in referrals for harder-to-reach patients?
- How many referrals were for new patients vs. closed cases where new barriers arose?
- Are there any trends that could help predict future SDOH needs?
CareAllies plans to continue to analyze available data to help answer questions like these to help shape the future of the program. In the meantime, the team continues to build relationships in the community and partner with providers to improve patient care.
85%
Rate of successful engagement through outreach to patients
97%
Rate of social needs met for participating patients

Mallory Kirby
Director, Health plan research
Posted on September 27, 2022
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox