Auto logout in seconds.
Continue Logout
This strategy report outlines five actionable priorities to improve bladder cancer care across health systems. It also focuses on patient education, care coordination, referral pathways, provider knowledge, and program measurement. The report addresses the challenges posed by high recurrence rates, complex patient populations, and evolving therapies, highlighting the need for standardized, guideline-concordant care.
Methodology
This project examined key strategies to improve bladder cancer care. To support this work, Advisory Board conducted eight hour-long interviews with bladder cancer care providers, including an oncodermatologist, a clinical pharmacist, and an oncology nurse, each representing eight health systems across the East Coast and Midwest United States. Participating organizations included academic medical centers and nonprofit multispecialty health systems.
Read on for key insights from the research team’s comprehensive literature review and interviews. For each strategy, the team outlines key insights, supporting evidence, additional resources, and guidance to help bladder cancer programs improve quality of care.
The challenge
Bladder cancer is a complex disease that requires ongoing management across multiple care settings, particularly in its regional and metastatic forms. It is the ninth most common cancer globally and the sixth most common among men.1 Regional bladder cancer accounts for about 7% of cases with a five-year survival rate of around 40%, while distant metastatic bladder cancer comprises 6% of cases and carries a survival rate of just 9%.2 These advanced stages often emerge after recurrence and are rarely curable, shifting treatment toward life-extending therapies.2
Disparities exist across age, gender, and race
Bladder cancer disproportionately affects older adults, with a median age at diagnosis of 73 and the highest incidence among individuals aged 65 to 74.3 Patients often present with complex comorbidities and chronic conditions that complicate care planning. Providers often conduct additional assessments, including evaluations of frailty, cognitive function, and treatment tolerance. These assessments can delay treatment decisions and contribute to variation in first-line treatment when patients are considered too vulnerable for standard therapies.
Bladder cancer is more common in men, who are nearly four times more likely to be diagnosed than women.3 However, women often present with more advanced disease and experience poorer outcomes.4 Racial and socioeconomic disparities further compound the burden. Black patients are less likely to receive guideline-concordant care and more likely to experience delays in diagnosis and treatment compared to white or Hispanic patients.4
4x
More common in men than women*
* See endnote 3.
High recurrence rates complicate treatment
Recurrence is a defining characteristic of bladder cancer and a critical factor in shaping care strategies. Recurrence rates can reach up to 50% among patients who initially respond to treatment, whereas recurrence rates of 5% are considered high for many other cancers.5 These recurrences often happen within the first four years.5
50%
Recurrence rate*
* See endnote 5.
Recurrence increases patient volume and heightens demand for follow-up care, coordination, and long-term monitoring.5 Patients may also experience increased emotional burden as they navigate decisions between extending life and maintaining quality of life.
Evolving therapies and increasing prevalence of adverse events
New treatments have been accompanied by a rise in adverse events (AEs), including skin reactions, peripheral neuropathy, and nephritis. These events complicate clinical management and may lead to inappropriate treatment discontinuation.6 This challenge is compounded by rapid changes in treatment guidelines and the continuous emergence of new therapies and clinical trials. General oncologists must stay current across multiple tumor types while also maintaining awareness of a wide range of potential adverse events and appropriate management strategies.
Bladder cancer carries a high financial impact on patients and the overall healthcare system
The economic impact of bladder cancer is considerable. Total annual costs exceed $6.5 billion, driven by direct medical expenses, indirect costs, and productivity losses.7 Among cancers, bladder cancer ranks among the highest in lifetime treatment costs because of its high recurrence rate and the need for ongoing surveillance.8 Care teams may coordinate proactively to prevent costly and resource-intensive hospitalizations and emergency department visits.
$6.5B
In total economic impact*
* See endnote 6.
Financial toxicity is also a significant concern for bladder cancer patients, particularly in later stages when complex treatment regimens, frequent appointments, and multiple providers contribute to high costs.7 This challenge is amplified by Medicare coverage gaps, including limitations for newer drugs and high out-of-pocket costs under Medicare Part D.7
5 strategies to improve bladder cancer care
Bladder cancer places a burden on the health system because of its high recurrence rates and complex patient population.5 The disease often affects older adults with multiple comorbidities, who typically fall outside the standard clinical trial model, making treatment planning and care coordination more challenging.
Health systems should prioritize key areas where care varies from guideline-concordant practice. Incorporate the following five strategies into bladder cancer programs to ensure patients receive timely, comprehensive, and equitable care.
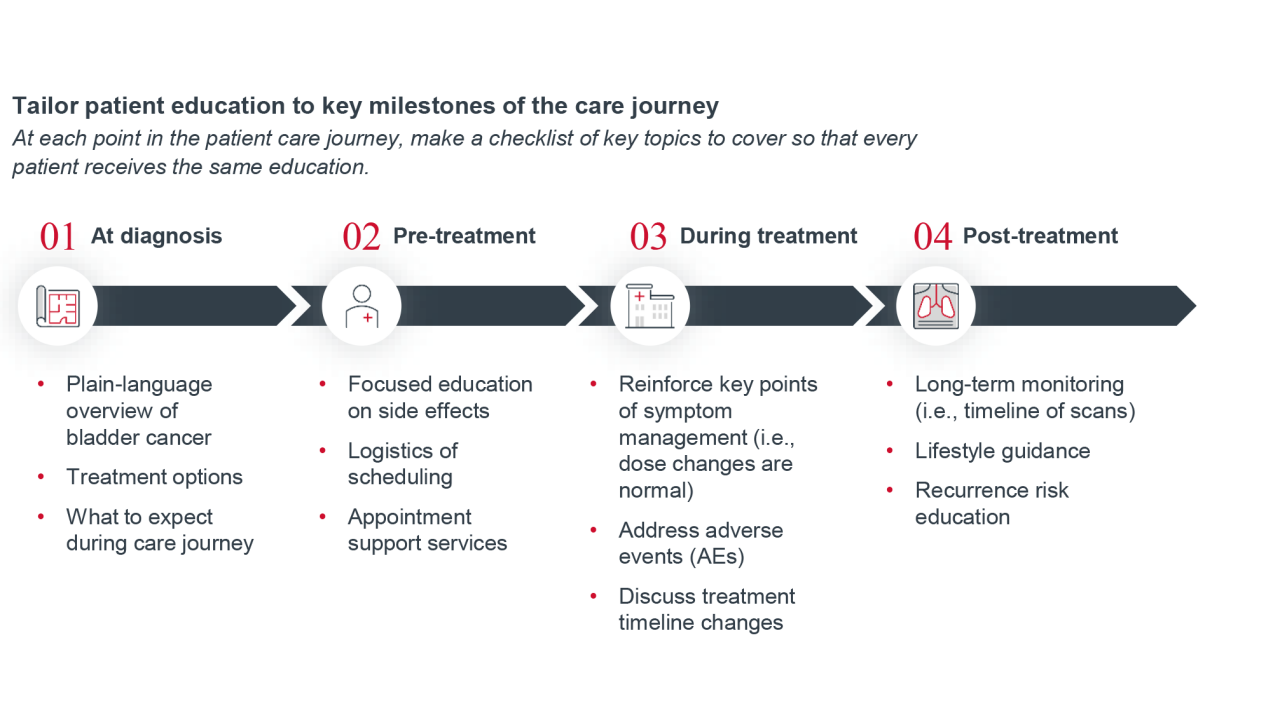
Oncologists should build trust with patients from the onset of diagnosis through treatment completion given the complex care journey and high recurrence rate of bladder cancer. A key step is to standardize patient education at specific timeframes during the care journey. This helps ensure that every patient understands their treatment plan, is aware of risk factors, and feels comfortable sharing concerns about side effects and complications that may arise during the treatment plan.
Patient check-in questionnaire or electronic Patient-Reported Outcomes
To encourage patients to raise concerns early and consistently, use a questionnaire at pre-determined points in the care journey. To develop these questionnaires, brainstorm the most common patient milestones and side effects and prioritize them based on typical patient experiences. For example, a questionnaire for the first month check-in might focus on medication side effects and the patient’s emotional well-being. Consider what the milestones are for subsequent visits and how the patient-reported outcomes can be collected electronically.
Sample of patient-reported outcomes for bladder cancer patients include:9
- Abdominal pain
- Constipation
- Diarrhea
- Decreased appetite
- Fatigue
- Insomnia
- Nausea
- Neuropathy
- Rashes
- Shortness of breath
- Swelling
- Urinary symptoms
Delineate roles and responsibilities across the care team
In a setting of high patient volumes and unique care needs, it can be difficult to make sure every patient receives an equal level of education during their bladder cancer care journey. To mitigate missed steps and bias, delineate role responsibilities among the care team. This will also ensure that no individual is overburdened with the task of education or follow-up questions. Clearly define each team member’s role and responsibilities so that every patient’s education is comprehensive and works in tandem to reinforce critical information throughout the care journey.
Example care team responsibilities




Additionally, consider the role of non-clinical staff. What is their responsibility, and at what points during the care journey is that responsibility important? For example, a social worker or financial counselor will address needs related to social drivers of health, such as transportation to appointments and filing insurance claims correctly.
Key performance indicators for patient education
- Patient-reported outcomes (PROs): Track symptoms, functional status, and treatment side effects
- Quality of life (QoL): Physical, psychological, and economic well-being
- Patient satisfaction: Net promoter score (NPS) or other satisfaction surveys
Patients often feel overwhelmed by the complexity of bladder cancer care, which involves tracking numerous appointments, tests, and treatment decisions. In addition to patient education sessions, care teams should also guide patients through each phase of care to reduce delays, minimize variation, and ensure timely interventions.
To keep patients on track, care teams should help them meet critical milestones and avoid missing appointments. Creating a patient journey map allows care teams to visualize the care path with patients, coordinate effectively, and ensure no patient falls through the cracks.
Care journey map
A care journey map allows providers to better track patients across key milestones and promotes standardization of treatment selection and continuation. The journey map should reflect the unique needs of a hospital or health system and should updated as recommendations evolve to promote guideline-concordant care. This approach helps providers consistently select appropriate first-line therapies and maintain alignment with evidence-based standards. The following offers a foundation to build a care journey map within bladder cancer care, along with key considerations for each phase of treatment.
Real-time tracking can monitor patient progress and flag opportunities for intervention
Teams should embed integrated tracking mechanisms within the standardized care journey framework to monitor patient progression, identify delays in care delivery, and assess adherence to treatment protocols.
Tracking patient milestones through digital platforms and integrated patient portals enables timely identification of critical transitions in bladder cancer care. Key milestones include initial diagnosis, referral to appropriate specialists, and initiation of treatment. By embedding structured data fields and alerts online, care teams can monitor progress and flag overdue actions — such as delayed referrals, missing consults, no-show appointments, or uninitiated therapies. Automated prompts and dashboards can highlight gaps in care and ensure that patients are not lost between stages.
Foundations of a care journey map
| Phase of treatment | Sample stakeholders | Sample responsibilities | Key considerations |
|---|---|---|---|
| Awareness & diagnosis |
|
|
|
| Staging & initial treatment |
|
|
|
| Monitoring & adverse event management |
|
|
|
| Survivorship & palliative care |
|
|
|
Dedicated care navigators promote continuity and personalized support
Assigning dedicated care navigators to each oncologist is a targeted strategy to enhance continuity and personalized support throughout the bladder cancer care journey. These navigators are responsible for tracking patient referrals and follow-ups, coordinating diagnostic testing and appointments, and serving as a contact point for patients for education and concerns.
By embedding navigators into the care team, organizations can proactively identify delays or gaps in care — such as missed consults or uninitiated therapies — and intervene before they impact outcomes. Dedicated care navigators can use the care journey map and real-time tracking to promptly identify patients who fall behind in their care pathway. They can investigate the underlying cause — such as missed appointments due to transportation barriers — and connect patients with appropriate support services, like arranging transportation, to resolve the issue and restore continuity in care.
This role supports operational efficiency by streamlining communication across specialties and ensuring that patients remain engaged and informed. Care navigators serve as a consistent point of contact, helping patients navigate complex care pathways and reinforcing adherence to guideline-concordant treatment plans.
Key performance indicators for patient journey mapping
- Missed appointment rate: Serves as an indicator of potential access barriers or patient engagement challenges.
- Treatment plan adherence: Measures completion of recommended therapies and consistency in following prescribed care.
Bladder cancer care involves a wide range of specialists and support staff who each contribute to different aspects of the treatment journey. Coordinating care across these roles can present challenges. Providers and care teams often struggle to collaborate consistently and share timely updates, making it difficult to monitor patient progress and maintain clear communication throughout the continuum of care.
To reduce delays and friction, care teams should establish sustainable communication structures that support real-time information exchange. These systems enable teams to work together more effectively and ensure that the patient journey map functions as intended.
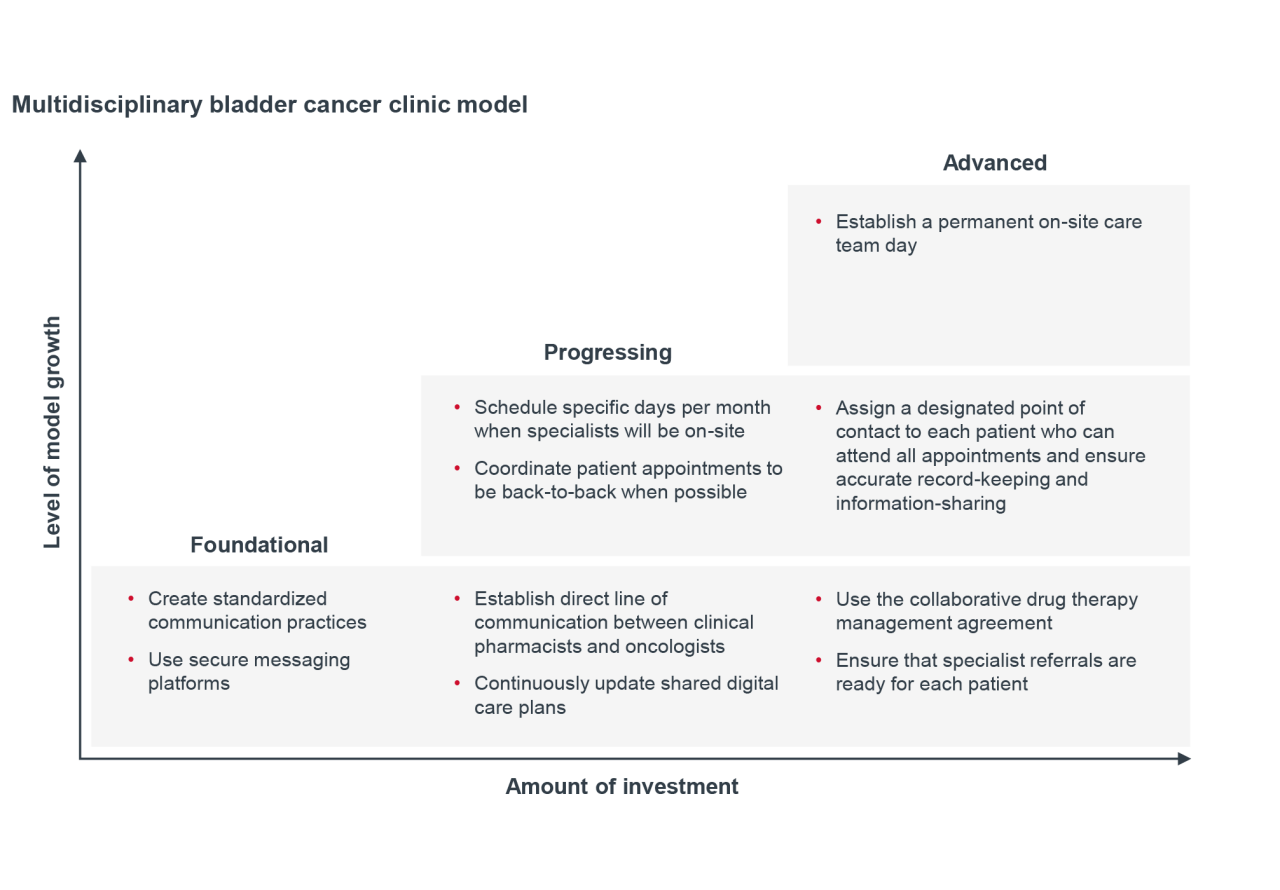
Build communication frameworks and protocols
A multidisciplinary team communication framework can improve real-time collaboration among providers involved in bladder cancer care. Standardized communication protocols can include the use of shared digital care plans that are continuously updated and accessible to all team members, enabling quick visibility into patient status and treatment progress. Care teams use secure messaging platforms to relay timely updates on treatment changes, referrals, and diagnostic results, helping reduce delays and miscommunication across specialties. Embedding these tools into routine workflows ensures that every care team member has a clear and efficient way to communicate with one another at any point in the patient’s treatment journey.
Collaborate with clinical pharmacists
Clinical pharmacists play a critical role in bladder cancer management by developing individualized treatment plans, optimizing dosing strategies, and anticipating potential side effects. Establishing a direct line of communication between the provider and clinical pharmacist can help ensure timely updates to the treatment plan as the oncologist communicates the need for changes.
Consider using collaborative drug therapy management (CDTM), a formalized agreement between clinical pharmacists and providers. Recognized in all 50 states and authorized in 46, CDTM enables pharmacists to manage treatment within defined protocols, including ordering labs and adjusting medications based on patient response. This formal agreement can help reduce delays in treatment adjustments and promote more coordinated medication management.
Key performance indicators for care team coordination
- Treatment plan adherence: Measures completion of recommended therapies and consistency in following prescribed care.
- Wait times: Tracks the duration from referral to first appointment and from diagnosis to treatment initiation, reflecting system efficiency and responsiveness.
The introduction of newly approved therapies into national guidelines creates new opportunities for patient treatment but also may increase adverse events. Hospitals and health systems need robust referral pathways that allow them to quickly adapt to new therapies and adverse events that their bladder cancer patients are experiencing.
Consider a decision tree to manage adverse events
Adverse events (AEs), particularly those related to infusion therapies, are common during a bladder cancer patient’s treatment journey. Lack of effective AE management can lead patients to delay or discontinue care.6
A decision tree standardizes the management of common AEs, which can allow care teams to efficiently triage. To create this decision tree, first identify common AEs (such as rash, diarrhea, fatigue, or neuropathy)6 for the first line therapies of bladder cancer. For each AE, create a severity scale identifying the symptoms that bucket it into a low, medium, or high priority. Depending on the priority rating, identify moments to trigger referrals to specialists that have been pre-identified as equipped to manage the AE within the hospital or health system. Include the referral specialists in the creation of the decision tree to gain buy-in for appointment priority.
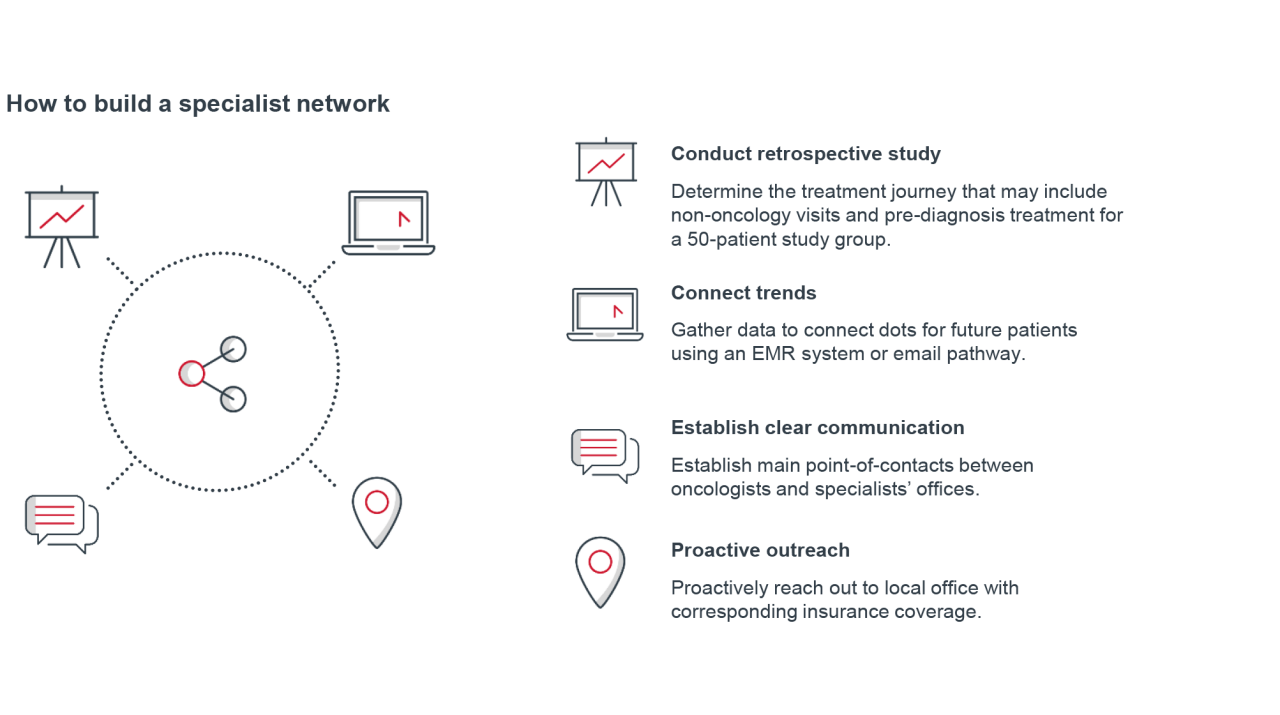
Build a network of specialist providers
Bladder cancer patients have a large care team that can include the medical oncology team, the urologist who identified the initial abnormality, and specialists who treat severe adverse events during treatment. While time intensive, a concerted effort to create a network of trusted specialists associated with the oncology practice may help improve patients’ treatment management and overall outcomes. Create and maintain a curated list of local and virtual specialists that the medical oncology team can lean on regularly.
Oncoderm Referral System
To ease the burden of access for cancer patients in need of dermatology care, a large health system created an e-mail listserv that enables oncologists to directly refer patients.10 The health system identified that cancer patients were not receiving timely dermatologic follow-up care due to digital platform related communication gaps and long appointment wait times. Creating this e-mail listserv specific to the oncodermatology referral pathway within the health system significantly improved scheduling efficiency.
A retrospective analysis showed:
- A decrease in average referral-to-scheduling time from 19 to 4 days.10
- A decrease in referral-to-appointment time from 51 to 22 days.10
Key performance indicators for enhancing referral pathways
- Emergency department visits/preventable admissions: Especially within 30 days of treatment
- Referral timeliness: Time from primary care or urology referral to specialist consultation
Improving the dissemination of clinical guidance and therapy updates is essential to ensure that all providers, including general oncologists who treat bladder cancer infrequently, deliver guideline-concordant care. Given the rapid evolution of bladder cancer therapies, numerous clinical trials, and frequent updates to care guidelines, clinicians may struggle to stay current amid their busy patient schedules. Four opportunities to equip providers with timely, digestible access to evolving clinical information include:
Create a physician champion model
A physician champion can be a dedicated physician or a rotating role charged with curating and sharing updates. This allows for other providers to receive timely, digestible information on evolving therapies and clinical guidance. Dissemination channels may include monthly article club summaries, biweekly email digests, and short internal video explainers.
Some organizations use a population health staff member dedicated to oncology. This individual curates information on new therapies, evolving care guidelines, and real-world treatment patterns, ensuring that frontline providers remain informed and aligned with best practices.
Use a centralized resource hub
A digital repository — such as a SharePoint site — can house key resources, including summaries of new therapies, decision trees for patient case management, and FAQ-style guidance documents. This hub enables providers to access up-to-date clinical information in a streamlined format, reducing reliance on fragmented or outdated materials. Regular updates aligned with evolving guidelines ensure that the content remains current and supports guideline-concordant care.
Encourage peer to peer collaboration
Peer-to-peer collaboration can help improve clinical consistency and knowledge-sharing across bladder cancer care teams. A formal network connects specialists, such as those involved in clinical trials or research with generalist providers, to help bridge gaps in guideline adherence and therapeutic awareness. This model supports the dissemination of real-world insights and emerging data. Collaboration models may already exist at the health system for other cancer types or diseases; consider applying the similar models to bladder cancer.
Establish a pharmaceutical liaison
A pharmaceutical liaison role strengthens the connection between providers and drug manufacturers. This liaison serves as a centralized contact point for reaching out to the drug manufacturer’s drug representatives and medical science liaison (MSL). The MSL can provide more in-depth information about therapies like guidance on dosing for non-clinical trial patient profiles and rare treatment toxicities.
In addition to clinical insights, the pharmaceutical liaison can proactively request tear-away pages or quick-reference materials from drug reps for newly approved therapies that may be relevant to patients. A one-pager summarizing the drug’s package insert is easier for patients to digest — making it a valuable tool for care team coordination and patient education.
Key performance indicators for addressing knowledge gaps
- Adherence to treatment plans: Including achievement of therapeutic milestones.
- Use of guideline-concordant care:
- Percentage of eligible patients receiving 1st-line (1L) therapy.
- Percentage receiving 1L maintenance therapy when indicated.
Measure progress of bladder cancer programs
To narrow the areas of opportunity, assess the following key performance indicators (KPIs) within the bladder cancer program. Identify the KPIs with the highest need for improvement, align to a strategic priority outlined in this report, and bring the need to leadership teams to improve care gaps.
Key performance indicators outlined in this report
- Patient-reported outcomes (PROs): Track symptoms, functional status, and treatment side effects.
- Quality of life (QoL): Physical, psychological, and economic well-being.
- Patient satisfaction: Net promoter score (NPS) or other satisfaction surveys.
- Missed appointment rate: Serves as an indicator of potential access barriers or patient engagement challenges.
- Treatment plan adherence: Achievement of therapeutic milestones and consistency in following prescribed care.
- Wait times: Tracks the duration from referral to first appointment and from diagnosis to treatment initiation, reflecting system efficiency and responsiveness.
- Emergency department visits/preventable admissions: Especially within 30 days of treatment.
- Referral timeliness: Time from primary care or urology referral to specialist consultation.
- Adherence to treatment plans: Including completion of recommended therapies.
- Use of guideline-concordant care:
- Percentage of eligible patients receiving 1st-line (1L) therapy.
- Percentage receiving 1L maintenance therapy when indicated.
1 GLOBOCAN 2022: Bladder Cancer 9th Most Common Worldwide. World Bladder Cancer Patient Coalition. February 14, 2024.
2 Cancer Stat Facts: Bladder Cancer. National Cancer Institute. Accessed March 18, 2026.
3 Saginala K, et al. Epidemiology of Bladder Cancer. Medical Sciences. March 13, 2020.
4 Castellon-Lopez Y, Thompson PA. Achieving health equity in bladder cancer care: Addressing disparities through collaborative research and evidence-based strategies. Bladder Cancer. December 23, 2024.
5 Ma, J, et al. Long-term Recurrence Rates of Low-risk Non–muscle-invasive Bladder Cancer — How Long Is Cystoscopic Surveillance Necessary? European Urology Focus. March 8, 2024.
6 Brower B, et al. Managing potential adverse events during treatment with enfortumab vedotin + pembrolizumab in patients with advanced urothelial cancer. Frontiers in Oncology. April 22, 2024.
7 Clark O, et al. Economic Impact of Bladder Cancer in the USA. PharmacoEconomics - Open. August 18, 2024.
8 Sievert KD, et al. Economic aspects of bladder cancer: what are the benefits and costs? World Journal of Urology. March 7, 2009.
9 Taarnhøj G, et al. Patient-reported outcomes item selection for bladder cancer patients in chemo- or immunotherapy. August 22, 2019.
10 Powers CM, et al. Access to dermatologic care for cancer patients: employment of an oncodermatology referral system. Supportive Care in Cancer. February 7, 2025.
At Pfizer, we’re in relentless pursuit of breakthroughs that change patients’ lives. We innovate every day to make the world a healthier place.
Our unique resources allow us to do more for people. Using our global presence and scale, we’re able to make a difference in local communities and the world around us.
Pfizer supports the global healthcare community’s independent quality improvement initiatives to improve patient outcomes in areas of unmet medical need that are aligned with Pfizer’s medical and/or scientific strategies. For more information, please visit www.pfizer.com.
This report is sponsored by Pfizer, an Advisory Board member organization. Representatives of Pfizer helped select the topics and issues addressed. Advisory Board experts wrote the report, maintained final editorial approval, and conducted the underlying research independently and objectively. Advisory Board does not endorse any company, organization, product, or brand mentioned herein.
To learn more, view our editorial guidelines.
This report is sponsored by Pfizer. Advisory Board experts conducted the underlying research independently and objectively.
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox