Auto logout in seconds.
Continue LogoutIn a past webconference, "How Heath System Pharmacy Leaders Are Reducing Employee Health Benefit Costs," we highlighted three key ways that health system pharmacy leaders are helping HR leaders lower costs while providing high quality pharmacy benefits to system employees and beneficiaries.
After the presentation, we had the opportunity to speak further with Colleen Mahoney, a pharmacist by trade and managing director at Advisory Board, who works with health systems on pharmacy benefit optimization for their employees and beneficiaries. We asked Colleen our members' most pressing questions on what pharmacy leaders need to know and do to demonstrate value. We’ve summarized our conversation below.
On working with HR leaders
Q: How should pharmacy approach their benefits team if they have yet to be invited to conversations around employee pharmacy benefits?
Colleen Mahoney: When I first started working with health systems, very few had a pharmacist involved in the pharmacy benefit manager contracting and negotiations processes. Now, it is becoming increasingly common.
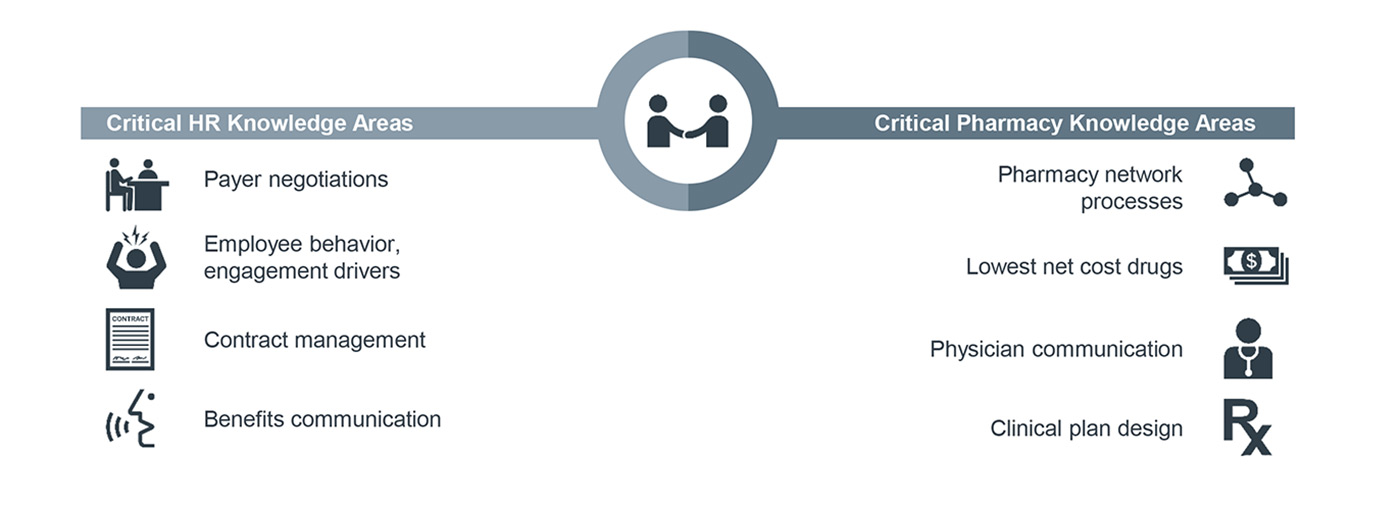
In cases where HR leaders are not yet asking for pharmacy’s input, pharmacy leaders should start by asking HR for a lesson in benefit management to demonstrate interest in collaboration and to better understand employee benefits. As the collaboration develops, pharmacy leaders can help the organization pursue three key opportunities to lower costs of care:
- Using an in-house pharmacy to reduce prescription copays and improve generic utilization among beneficiaries
- Aligning formularies between clinics, hospitals, and employee plans to better control medication utilization and prescribing patterns for employees
- Improving benefit discussions and pharmacy benefit manager (PBM) contract negotiations by filling gaps in HR knowledge around pharmacy topics
On integrating clinical services
Q: How are organizations integrating their PBM management with medication therapy management (MTM) and clinical services?
CM: One tactic I've seen organizations take is to collaborate with the PBM's diabetes coordinator or disease management staff to identify and create action plans for high-risk patients within the system. This includes referring patients to in-house MTM services for counseling on appropriate medication use and to conduct a full medication review to identify areas for medication reconciliation. These programs often focus on diabetes, hypertension, high cholesterol, asthma, or congestive heart failure.
For more information on how organizations have integrated pharmacy into these primary care programs, check out our research briefing, Integrated Pharmacy Models in Primary Care, which outlines five case study examples.
On working with health system employees
Q: How can systems ensure that plan changes are appropriately communicated to their employees to manage and mitigate problems that may arise?
CM: I have seen employee communication handled in a variety of ways. Leading organizations use a combination of strategies to get the message across:
- Announcement letters: Employers can either send a notification of changes directly to employees or employers can ask their PBM to draft a letter for their review and approval to send from the PBM to employees. It's also helpful to reinforce the message by mentioning changes in employee newsletters.
- In-person meetings: Organizations should leverage department-level meetings and their benefits fair to review all plan changes and answer any questions.
- Personal phone calls and help lines: All organizations should communicate a telephone number that employees can call to address issues and concerns. Some take this a step further and use personalized phone calls to counsel patients who are impacted by plan changes.
In all cases, it is essential that health systems and their PBMs communicate their strategy and plan design changes to ensure a smooth implementation for the members.
Q: What does it take to switch employees to an in-house pharmacy? What incentives and co-pay structures are most effective?
CM: When thinking about serving the employees in the organization, health systems must focus on convenience and price to influence behavior. They can then gradually implement stricter requirements based on employee tolerance for change. Many hospitals begin by lowering copayments for in-house fills or raising the copayment for prescriptions filled outside of the system. Some hospitals use mail-order services to provide coverage and convenience across large geographic spans.
The most effective approach to move employees to the in-house pharmacy is to require maintenance medications be filled in-house after the first two, 30-day fills. One organization that implemented this tactic raised their in-house fill rate from 30% to 68% in three months.
On working with PBMs and brokers
Q: How can organizations reduce spread generated by PBMs and improve rebate pass through?
CM: The bottom line here is that organizations must develop the most transparent PBM contract possible and that they must have that PBM audited regularly to ensure contract compliance and continued transparency. This will ensure that the hospital is receiving all discounts and rebate guarantees placed in the contract.

Organizations can use two additional contract mechanisms to manage spread and rebates: First, they can restrict contract language so that there is only one possible MAC (maximum allowable cost) price list for purchasing and charging; and second, they can mandate that the PBM pass through 100% of all manufacturer derived revenue.

Posted on January 25, 2018
Updated on March 17, 2023
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox