Auto logout in seconds.
Continue LogoutEditor's note: This popular story from the Daily Briefing's archives was republished on April 5, 2019.
Read Advisory Board's take on this story.
Doctors may be using outdated guidelines that overestimate—and in some cases underestimate—a patient's risk for heart attack or stroke, as well as the patient's need for preventive medications, according to a study published this summer in Annals of Internal Medicine.
Researchers posted an updated calculator online.
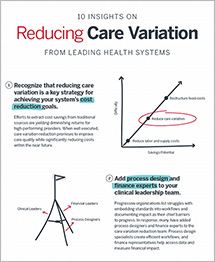
The CV guidelines library
Kickstart your care variation reduction strategy with our suite of guidelines and care standards
About the study
For the study, researchers at Stanford University examined a commonly used risk calculator that doctors can access online or in EHRs to determine a patient's 10-year risk for cardiovascular disease. That calculator, which launched in 2013 and is endorsed by the American College of Cardiology and the American Heart Association, is based on statistical analyses that combine data from a number of large studies.
But Sanjay Basu, assistant professor of primary care outcomes research at Stanford and the senior author of the new study, said in his practice he discovered the calculator's risk estimates often didn't match the actual risks of patients he was seeing, especially his African-American patients. According to Cooney, few African-Americans were included in the studies used to create the 2013 calculator, which led to a statistical overgeneralization for that population.
To address this, Basu and his team applied newer statistical tools—such as machine-learning techniques used to determine which YouTube videos consumers are more likely to watch—to newer and more racially and ethnically diverse data sources. Regarding his use of machine-learning technology, Basu said, the goal is the same for cardiovascular risk prediction as it is for what YouTube video a consumer may prefer: identify subtle characteristics and relationships that, in this case, could result in an increased risk of heart attack and stroke.
The researchers compared the results to data that showed whether those people actually had a heart attack or stroke over the next 10 years.
Findings
The researchers said the updated model correctly reclassified 13 people as low risk for every one person it classified incorrectly. Based on those results, the researchers estimated about 11.8 million U.S. adults may have inappropriately been deemed high-risk and prescribed medications to reduce that risk.
The researchers also found the updated model addresses the discrepancies Basu discovered in his daily practice. The original calculator often projected drastically different risk estimates for African Americans with the same health characteristics, with rates ranging from a 70% lesser risk of a heart attack or stroke than whites to a 250% increased risk—something that is highly implausible, according to Basu. However, the updated model showed fewer than 1% of African Americans had those implausible risk estimates.
"We found that a person's risk might be higher than previously believed and in other cases might be much lower," Basu said. However, he said the updated model needs to be evaluated by independent researchers and then tested in clinical settings before it could be adopted.
Discussion
Nancy Cook, a professor of medicine from Harvard Medical School at Brigham and Women's Hospital, said the new model "is a move in the right direction," adding that she believes it to be "a more accurate model" than the original 2013 calculator, as it's "calibrated better, and the estimated risk fit the observed risk better."
In an editorial accompanying the study, Andrew DeFilippis and Patrick Trainor of the University of Louisville, wrote that the creation of the new calculator "is timely because a growing Hispanic population and 40% increase in Asian-Americans account for more than half of the U.S. population growth between 2000 and 2019." However, they wrote that the updates likely do not account for the way race could change an individual's risk of heart attack or stroke.
Donald Lloyd-Jones, chair of the department of preventive medicine at Northwestern University and the co-chair of the task force that created the original 2013 calculator, said the Stanford researchers had "applied some very interesting and new methods about how we can improve risk equations. And this is what should happen."
Ultimately, Basu said risk calculators should not be the end all be all for a patient's treatment decisions. He said the choice of treatment should be "a personal decision between the patient and doctor based on a number of factors" (Cooney, STAT News, 6/4).
Advisory Board's take

Megan Tooley, Practice Manager, Cardiovascular Roundtable
This study highlights a problem many CV programs face: how to reduce care variation while also providing tailored care to each patient. The service line is fortunate to have a robust library of clinical guidelines, appropriate use criteria, and consensus statements. However, this and other recent studies have found that many of the trials behind these guidelines did not adequately account for diversity of race or gender, nor for sociodemographic risk factors. As a result, they may not be appropriate for use with all patients. Programs must, therefore, carefully evaluate patient-specific characteristics when putting care standards into practice.
Risk algorithms can be helpful tools for guiding care management and treatment decisions, but they are just that: tools. In speaking with programs that have successfully reduced unwarranted care variation, we've heard how important it is to give clinicians the opportunity to adjust care decisions based on a patient's unique characteristics and their own judgement.
One organization we spoke to used manual EMR overrides to strike this balance. They embedded a risk algorithm into the EMR-based admission assessment for all heart failure patients in order to identify high-risk patients who should be added to their care management panel. However, understanding that this algorithm is not infallible, they also added a simple override option for nurses to use if non-clinical factors, which were not incorporated into the algorithm (e.g., homelessness, recent traumatic life event), warrant additional care management services. Nurses have to clearly state what these characteristics are in order to proceed.
To learn more about the best practices we've discovered to reduce unwarranted CV care variation—while still allowing for clinician autonomy—read our research briefing on how to build your no-regrets CV strategy.
Ready-to-present slides: Cardiovascular market trends for 2019
Want the latest information for your next cardiovascular meeting? This ready-to-use presentation contains the Advisory Board's most popular slides on cardiovascular market trends, from growth outlook and financial considerations to new care management priorities and programmatic innovations.
Use the slides to frame your next cardiovascular meeting and build a strong foundation for your presentation.
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox