Auto logout in seconds.
Continue LogoutJohns Hopkins Medicine has boosted operational efficiency without adding staff by creating a new command center, which is expected to pay for itself within the next three years, Mandy Roth writes for HealthLeaders Media.
Get 10 market perspectives and operational priorities for AMC leaders
Background
Johns Hopkins Medicine annually handles more than 115,000 inpatient admissions and 360,000 emergency visits at the health system's six academic and community hospitals, which have a total of 2,671 beds.
Jim Scheulen, chief administrative officer for emergency medicine and capacity management at Johns Hopkins Medicine, said that before Hopkins launched the command center, the team "realized that we were managing an incredibly, incredibly complex operation, trying to manage the flow of thousands of patients through our system safely with high-quality outcomes."
Scheulen added, "When there is a mismatch between supply and demand, you see wait times where you don't want to see them. It played out in our inability to bring in as many patients as we thought our [tertiary referral center] should handle."
Launching a command center
To address its capacity challenges, Johns Hopkins Medicine in 2016 established the Judy Reitz Capacity Command Center, a 5,200-square-foot hub, together with GE Healthcare Partners. Johns Hopkins Medicine did not hire additional employees to launch the center.
The health system did not disclose the cost of developing the command center, but costs for technology solutions from GE Healthcare Partners can range from $5 and $20 million for consulting fees, construction, and IT expenses, Roth reports.
The center's walls are lined with large digital screens that display real-time dashboards to employees at 38 workstations. The command center aggregates data derived from 15 IT systems and uses artificial intelligence and predictive analytics "to create a more accurate picture than a single software solution or device can deliver," Roth reports.
The center is responsible for every patient who becomes part of the health systems through Hopkins Access Line (HAL), which handles referrals for transferring a patient, and Johns Hopkins Lifeline, which dispatches transport teams for critical care.
Signs of success
Scheulen said that over the course of nearly two years, the command center has helped the health care system become more effective. According Scheulen, since implementing the command center, Johns Hopkins Medicine has seen:
- ED boarding reduced by 20%;
- OR holds decline by 80%; and
- Patient transfers from other hospitals increase by 60%.
Due to these improvements in operational efficiency, Scheulen said, "We've essentially created 16 additional beds of capacity, without actually opening 16 beds."
Scheulen shared four insights from his experience with the health system's command center:
1. Use the principles of system engineering to improve workflow.
According to Scheulen, the health system's command center allows Johns Hopkins Medicine to leverage the principles of systems engineering—an approach employed in the airline industry, among others—to take "an organized approach to improv[e]…[work]flow."
Scheulen said system engineering "means using advanced technology, like simulation and optimization modeling—heavy statistical analysis of data—and collocating all of the resources that have to do with managing your operations on a day-to-day basis."

Get your physician engagement in gear
For example, Scheulen said employees at the command center receive real-time information and monitor performance, such as patient outcomes and hospital bed capacity, much like an airline control center.
2. Simulate the effects of big changes—before you make them.
After the command center began operation, the team at Hopkins used simulation technology to explore the effects of different projects and processes. For instance, the technology allowed them to probe the combined effects of bed distribution and a reduction in the length of hospital stays on ED boarding, OR holds, and more. In this way, the team could determine which projects and processes would generate the best results for the health care system.
3. Engage clinicians early and often.
To engage leaders in the command center's work, the team at Hopkins used a two-pronged approach. First, they brought clinical leadership on board with the command center early in the development process. Second, they created a cross-functional team within the command center that included representatives from four departments: the physician referral service, critical care transport, admissions, and bed management teams.
Further, before a proposed system redesign or process improvement advances to executive leadership for approval, a clinical advisory panel reviews the proposal. Scheulen said, "Having clinical department leadership working with you (is) the right thing to do, and it's more likely to lead to success."
4. You don't have to build a whole command center to see benefits.
If a health system is interested in improving its efficiency, a command center might provide an advantage—but Scheulen said, in most cases, health systems don't have to create a complex new command center to see benefits. "Do you need the same level of complexity of a model that we built?" he said, adding, "Probably not. … Organizational strategy will drive what you do."
According to HealthLeaders Media, the technology Johns Hopkins Medicine uses is scalable for smaller health care facilities, but it is generally not an effective approach for hospitals with fewer than 200 beds (Roth, HealthLeaders Media, 6/7).
Primer series: How to address avoidable ED utilization
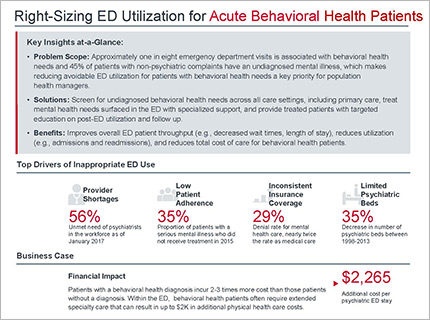
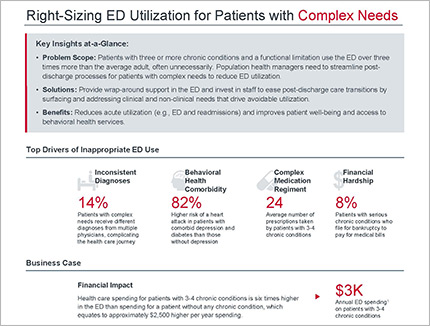
Are specific patient populations making up a significant proportion of avoidable ED visits at your organization? In each primer, we profile organizations who have set up targeted programs and feature operational, staffing, and funding information.
{kind=link}
{kind=link}
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox