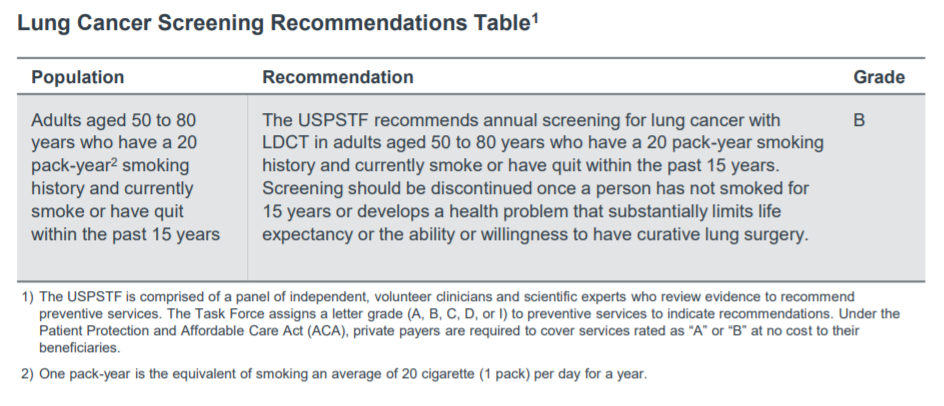
Auto logout in seconds.
Continue LogoutIn March 2021, the US Preventive Services Taskforce (USPSTF) approved highly anticipated revisions to lung cancer screening recommendations. This is the first update since 2013 when the Task Force initially recommended annual low dose computed tomography (LDCT) lung cancer screening exams for high-risk patients. The new guidelines nearly double the number of Americans eligible for the lung cancer screening. In particularly good news, the most dramatic increases are among populations with the highest lung cancer mortality and/or those at the highest risk for lung cancer at younger ages, that is, female, Black, and Hispanic patients.
How will lung cancer screening guidelines change?
The screening recommendation of annual LDCT exams remains, but who is eligible for those exams expand in two important ways:
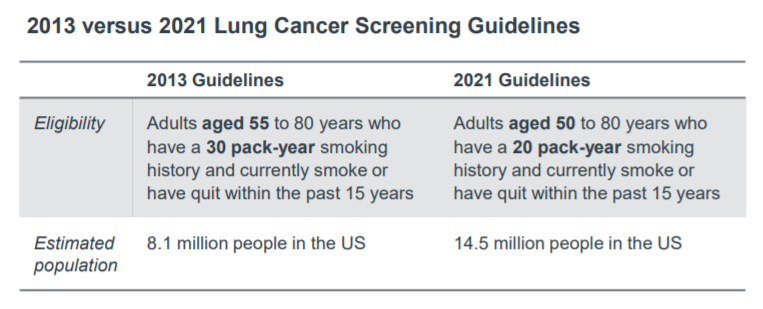
- To younger patients; eligibility will begin at age 50, down from age 55.
- To those with a shorter history of smoking, dropping the number of pack years from 30 down to 20.
Taken together, this increases the eligible population by 6.4 million people or by nearly 90%. The new guidelines have a notable impact on both racial minorities and women. Eligibility increased by 107% in Black adults and 112% in Hispanic adults compared to 78% for white adults, as well as 96% in women compared to 80% in men.
Lung cancer is the leading cause of cancer death in the US, accounting for nearly 25% of all cancer deaths. This is partially because patients with lung cancer may remain asymptomatic until late stages, reducing access to potentially curative treatment options. This increase in eligibility has the potential to improve lung cancer mortality. Based on new trial data and modelling studies, these guidelines could reduce lung cancer mortality by 13.0%, and thereby avoiding 503 lung cancer deaths and contribute to 6,918 life-years gained per 100,000 people.
The harsh reality of lung cancer detection today
Expanded eligibility for lung cancer screening is good news. But an increase in eligibility does not necessarily mean an increase in screening volumes. To meaningfully improve early stage detection, leaders must consider the broader context of lung cancer screening.
Lung cancer screening rates remain dramatically low.
In high-risk patients receiving LDCT screenings, clinical trials have demonstrated that annual screenings can reduce lung cancer mortality by 20%. Despite this, lung cancer screening rates remain low with only about 14% of eligible patients receiving the recommended screening exam versus 66% for breast cancer screenings and 69% for colorectal cancer screenings.
Why are screening rates so low? Here are a few of the most common reasons Advisory Board researchers hear from provider leaders:
- Patients, and even some referring providers, are unaware of the screening exam, eligibility, and clinical benefits, and/or have concerns about radiation exposure, overdiagnosis and false-positive scans
- Referring providers and screening programs struggle to track accurate smoking history
- Some patients are hesitant to receive the exam due to stigma around smoking and perceive lung cancer as a personal failure
- Due to geographic spread, some patients are unable to access lung cancer screenings
- Some high-risk and often lower income patients may struggle to cover screening costs out-of-pocket, as only private payers are required to cover the exam
Health disparities persist in lung cancer
Disparities3 in lung cancer screening and, subsequently, cancer outcomes persist. Lung cancer mortality is highest among Black men, and five-times higher among the least educated men compared to the highest educated men. Women also have a higher incidence of lung cancer than men.
Screening disparities can primarily be attributed to eligibility criteria that fails to account for differences in risk related to race, socioeconomic status (SES), or gender. For example, Black Americans, women, and low SES populations were more likely to be ineligible for screening, not meeting minimum age or smoking history criteria, despite demonstrating an overall increased risk for lung cancer.
USPSTF’s 2021 recommendation helps address some race and gender disparities. However, these new guidelines will likely have a limited impact on low SES populations due to differences between which insurance providers cover the cost of LDCT screening.
Insurance coverage doesn’t capture critical populations
USPSTF recommendations must be covered by private health plans, and Medicare almost always follows suit. However, Medicaid coverage for preventive services varies from state to state. In fact, only 31 Medicaid fee-for-service programs covered preventive lung cancer screening as of January 2019.
This leaves out two critically important, and often lowest income, populations: those that rely on Medicaid plans and those who are uninsured. This is especially important because belonging to a racial minority, low SES, and poor literacy all increase the likelihood of someone being uninsured. Even more, low SES is correlated with heavier use of cigarettes, making this population particularly important to target for early lung cancer detection.
Put simply, many patients that would benefit most from no-cost LDCT screenings will remain unable to access this potentially life-saving service.
Screening is only one piece of a comprehensive lung cancer detection program
While smoking remains the biggest risk factor for lung cancer, about 12% of diagnoses are in patients with no smoking history according to a recent study. These cases may be identified incidentally, when a pulmonary nodule is detected outside the primary purpose of the scan. In one cancer center, as many as 65% of the nodules referred to the program were detected incidentally versus through screening or presence of symptoms.
As such, we believe a comprehensive lung cancer program should involve two parts: screening and nodule management. To be successful, it is critical that nodule management programs be highly organized with clear and appropriate care pathways for patients with lung nodules to prevent patients from being lost between finding and follow up.
This approach enables programs to both reduce existing barriers to lung cancer screening and address health disparities by identifying patients outside of screening, such as during routine or emergent imaging procedures.
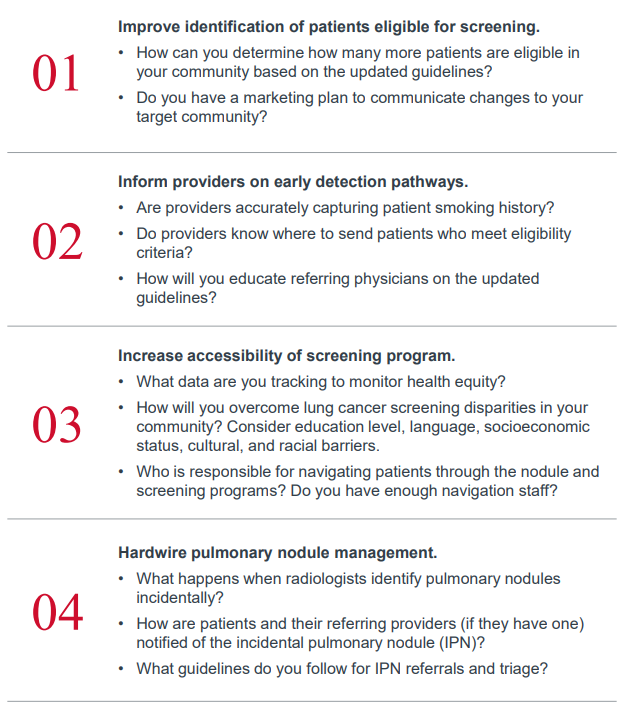
Advisory Board guidance and next steps
This content was developed by Advisory Board and does not express the views and opinions of AstraZeneca. It should not take the place of your clinical judgment. These are general recommendations for educational purposes only. Individual recommendations for patients may vary.
Click here to download this article in PDF format.
3Health disparities are defined as the higher burden of illness, injury, disability, or mortality experienced by one population relative to another. These differences are based on unnecessary, avoidable, or unjust socially determined factors including geographic location, race, ethnicity, gender, socioeconomic status (SES), and literacy.
Sources
American Lung Association. (2020). Lung Cancer Screening Coverage in State Medicaid Programs. Retrieved from Lung.org: https://www.lung.org/getmedia/cb086cfd-2fbb-4737-b518-e83cf1fcc411/lung-cancerscreening-1.pdf.
Centers for Disease Control and Prevention. (2021, March 2). Nation Center for Health Statistics. Retrieved from Data Finder: https://www.cdc.gov/nchs/hus/contents2019.htm
Henderson, L. M., Rivera, M. P., & Basch, E. (2021). Broadened Eligibility for Lung Cancer Screening: Challenges and Uncertainty for Implementation and Equity. JAMA, 325(10), 939-941. Retrieved from: https://jamanetwork.com/journals/jama/fullarticle/2777223?casa_token=vDE_-49eFhcAAAAA:21mF_MFCwy__aJNBTAOs0knaMbUZPeeCwLns-5AAsUZquj0EK22CUlK6i4pStqqpP7shtCt1yk2LZQ
Rivera, M. P., Katki, H. A., Tanner, N. T., Triplette, M., Sakoda, L. C., Wiener, R. S., ... & Aldrich, M. C. (2020). Addressing Disparities in Lung Cancer Screening Eligibility and Healthcare Access. An Official American Thoracic Society Statement. American journal of respiratory and critical care medicine, 202(7), e95-e112.
Siegel, D., & al, e. (2021). Proportion of Never Smokers Among Men and Women With Lung Cancer in 7 US States. JAMA Oncol, 302-304. Retrieved from: https://jamanetwork.com/journals/jamaoncology/article-abstract/2773380
US Preventive Services Task Force. (2021). Screening for Lung Cancer. Journal of the American Medical Association, 962-70.
Zahnd, W., & Eberth, J. (2019, Aug). Lung Cancer Screening Utilization: A Behavioral Risk Factor Surveillance System Analysis. Am J Prev Med, 250-255. Retrieved from https://pubmed.ncbi.nlm.nih.gov/31248742/US-52810
In Partnership with the Lung Ambition Alliance
The Lung Ambition Alliance, a global coalition with partners across disciplines in over 50 countries, was formed to combat lung cancer through accelerating innovation and driving forward meaningful improvements for people with lung cancer. We do this by advocating for improved approaches in three areas: screening and early diagnosis, accelerated delivery of innovative medicine, and improved quality care.
This report is sponsored by AstraZeneca, an Advisory Board member organization. Representatives of AstraZeneca helped select the topics and issues addressed. Advisory Board experts wrote the report, maintained final editorial approval, and conducted the underlying research independently and objectively. Advisory Board does not endorse any company, organization, product or brand mentioned herein.
To learn more, view our editorial guidelines.

Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox