Auto logout in seconds.
Continue LogoutExecutive Summary
The Hospital Readmissions Reduction Program (HRRP) adjusts hospital inpatient Medicare payments based on readmission rates of a set list of procedures. It is one of three mandatory pay-for-performance (P4P) programs that the Affordable Care Act introduced and is managed by the Center for Medicare and Medicaid Services (CMS). A readmission occurs when a patient returns the hospital for unscheduled inpatient care within 30 days of a prior stay. The program penalizes hospitals up to 3% of their inpatient Medicare revenue for having worse-than-average readmissions rates for six conditions listed below. Since the policy's implementation, readmissions rates have decreased for each condition, though some studies link the program to an unintended increase in mortality rates, calling into question the overall effectiveness of this program.
Why is the Readmissions Reduction Program a key issue for providers?
CMS introduced the HRRP to incentivize hospitals to reduce readmissions, which are a key driver of rising Medicare costs. Before CMS created this program, hospitals had little financial incentive to reduce readmissions as they were actually paid for each additional readmission. However, hospitals can now face penalties on the inpatient Medicare reimbursement for high readmission rates through both the HRRP, as well as the Hospital Value-Based Purchasing (VBP) Program.
How does the Readmissions Reduction Program work?
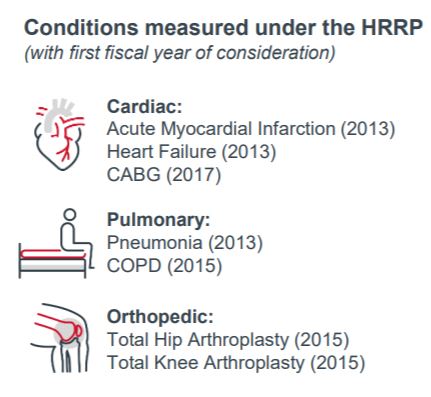
The HRRP measures and penalizes hospitals for worse-than-average readmission rates for heart failure, acute myocardial infarction (AMI), pneumonia, chronic obstructive pulmonary disease (COPD), coronary artery bypass surgery (CABG), and total knee/hip replacement (TKA/THA).
To determine readmissions penalties, Medicare first collects readmission data for a three year period prior to the year the penalty is assigned. For example, 2020 penalties are based on readmission rates from 2015-2018. As a result of the delayed three-year time frame, hospitals need to make a long-term commitment to reduce readmissions before their penalties can fall.
Next, CMS assigns hospitals to one of five peer groups based on their number of dual-eligible1 Medicare inpatient stays. A hospital’s performance is then compared to that of other hospitals within their peer group. If a hospital has a higher than average readmission rate for that group, they get a penalty.
Unlike Value-Based Purchasing, another Medicare P4P program, the HRRP does not offer monetary rewards for high performance.
How does the Readmissions Reduction Program affect providers?
Clinical
Readmissions occur for a variety of reasons. Some of these factors are unavoidable, such as the result of chronically ill patients needing frequent care. Other readmissions are due to hospital errors or subpar care and can be avoided. Many also result from patients failure to comply with medication, clinician instructions, follow-up care, or diet. Because the HRRP does not segment by the cause of readmissions, the program incentivizes hospitals to revamp discharge processes, improve compliance, and optimize treatment adherence. Beyond payment penalties, hospital reputations are also at stake, as readmission rates are published on CMS’s Hospital Compare website.
Financial
CMS consistently penalizes approximately 75% of hospitals for excessive readmissions. However, despite threats of these penalties, hospitals shoulder a financial burden associated with efforts to reduce readmissions, including discharge processes, follow-up phone calls, and home visits.
The HRRP also has an outsized financial impact on safety net hospitals. Hospitals which serve many low-income patients are 2.7 times more likely to have higher than average readmissions than hospitals in wealthier areas. However, starting in 2019, a new penalty methodology scraped a comparison of each hospital to a national standard. Instead, CMS now categorizes all participating hospitals into five cohorts according to the proportion of dual-eligible patients each hospital serves. Therefore, each hospital is compared to the median readmissions performance of its cohort, and hospitals with higher-than-cohort-median performance receive a penalty of up to 3%.
Operational
Hospitals are ramping up efforts to provide discharge instructions and post-discharge follow-up to ensure that patients comply with physician advice, fill prescriptions, and adopt a healthy lifestyle. Prior to discharge, hospitals must simplify their instructions to patients and develop better educational materials. Many hospitals turn to phone calls, emails, or text reminders to maintain contact with discharged patients. Some post-discharge efforts have included daily home food deliveries to encourage healthy eating, and employing social workers to hold daily meetings with high-risk patients.
How might the Readmissions Reduction Program impact provider-supplier sales relationships?
The HRRP plays a role in hospital budget discussions and affects hospital negotiating patterns. Hospitals may also change clinical and non-clinical processes to improve readmissions. Products and devices used within service lines like cardiology, pulmonology, and orthopedics will feel the most impact.
Readmissions-reducing products command a premium
- Vendors can develop internal data capabilities or partner with insurers to demonstrate how their products reduce readmissions. Implantable medical device companies in particular have an excellent opportunity to partner if their products reduce readmissions.
Patient compliance carries significant weight
- Suppliers can focus their natural business acumen and marketing skills to assist hospitals in promoting patient education, coordination across sites of care, and medication compliance.
Opportunity exists for supplier-provider risk-sharing
- Because HRRP penalties put a dollar value on each readmission, vendors willing to stake part of their contract on product performance can potentially differentiate themselves while helping their hospital customers.
Conversation starters with the hospital C-suite
- For what conditions are your readmissions highest? What is your reduction goal for this year? For the next three years?
- What clinical efforts have you undertaken to limit readmissions? What are the biggest obstacles you have faced?
- What challenges are you having with promoting patient compliance and healthy habits post-discharge?
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox