Auto logout in seconds.
Continue LogoutThe New York Times' Elisabeth Rosenthal this week examined why one of the simplest medical procedures—closing a wound with a needle and thread—now costs upwards of $500. Per stitch.
Rosenthal on health costs
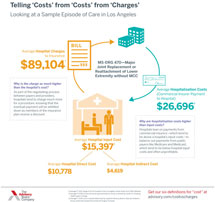
Economists say the primary driver of high health costs in the United States is fiscal, not medical. Hospitals hold significant negotiating clout in a health care system that has little-to-no price regulation, Rosenthal writes, noting that the rising costs of drugs, medical equipment, and other services—as well as fees from layers of middlemen—also play a significant role.
However, Rosenthal argues that an equally important factor behind escalating hospital bills is the growing number of mergers and consolidations that have led to supersized hospital systems, giving them the power to command higher prices from insurers and employers.
AHA makes the case for hospital mergers
Case study: The cost of three stitches and a dab of glue
Rosenthal offers the example of Deepika Singh, a 26-year-old woman who sought emergency care after gashing her knee at a barbeque. Singh's three stitches cost $2,229.11. Another patient, a rambunctious toddler named Orla Roche, sought care at the same ED after falling from a couch and splitting her forehead open. Sealing the wound with some skin glue cost $1,696.
The two patients were treated at one of two dozen community hospitals in the region owned by the same parent company, Rosenthal explains. At these hospitals, "chargemaster" prices for common procedures are among the 20% highest chargemasters in the country, according to a New York Times analysis of federal data.
Experts note that "chargemaster" prices are largely arbitrary and do not reflect what the patient actually pays, because public and private insurers negotiate discounts. The hospital that treated Singh and Orla charges $181 for a vial of skin glue, $126 for anesthetic cream, and $79.73 for a vial of local anesthetic. The same items can be purchased for $18, $37, and $5, respectively, on the Internet, according to Rosenthal.
Additionally, total billing for ED visits typically include separate charges for services and supplies, as well as a facility fee for walking in the door. For example, Roche's bill includes a $529 charge for "supplies and devices," while both her and Singh's total costs included a $1,167 facility fee.
The merger effect
Rosenthal writes that in theory, health care consolidation can create economies of scale and keep prices low—unless it results in complex super systems.
Typically, insurers will pay 40% to 50% of a patient's total bills, according to Simone Singh of the University of Michigan. However, powerful hospital chains are able to leverage their size to dictate higher prices than a typical hospital.
As such, discounts from the chargemaster prices can be less generous at super-systems, and patients like Singh and Orla end up paying more. For her three stitches, Singh's negotiated her $2,200 bill down to $1,813, and Singh had to pay $768.56 of that out of pocket, an amount she was unable to afford. Meanwhile, Roche's family ended up owing $1,366 after the insurer brought her bill down to $1,700 bill.
Longest article in TIME history explains high U.S. health costs
According to health care consultant Orry Jacobs, the effect of more hospital mergers and acquisitions ultimately depends on the objective of the health care system. "If the intent is to improve care and bend cost curves, then networks can do so. If the objective is to corner the market and demand higher rates, then that will happen" (Rosenthal, Times, 12/2).
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox