Auto logout in seconds.
Continue LogoutWelcome to the "Lessons from the C-suite" series, featuring Managing Partner Eric Larsen's conversations with the most influential leaders in health care.
In this edition, James Hereford, president and CEO of Fairview Health Services, talks to Eric about lessons learned on the ranch, a lifelong journey to "find the hard projects," and how 2017—which has already seen a health system merger, incorporation of a health plan, and negotiation of an academic medical group contract—is shaping up for Fairview.

James Hereford, President and CEO of Fairview Health Services
Question: James, your background is fascinating and, I think we can agree, unconventional. You grew up on a ranch in Montana, spent seven years as a high school math teacher and basketball coach, and now you're president and CEO of Fairview Health Services. You received your undergrad and graduate degrees in mathematics from University of Montana—
James Hereford: Let me stop you right there, Eric. It's Montana State. Now to those of us Montana State alumni, that is an important distinction.
Q: Er, let's try this again. Perhaps you can offer some reflections on how you went from a Montana ranch hand to the CEO of a $5.5 billion health system.
Hereford: I have to start with the key turning point in my career: I was six or seven years old, and my dad got me up in the middle of the night to check the cows during calving season, and he decided that was the night to teach me to 'turn a calf,' meaning assist with a breech birth on the ranch. It was one of those cold, snowy spring nights in Montana, and I just had this moment of incredible clarity—being there, up to my shoulders in cow, all kinds of fluids coming in my direction—that this was not what I wanted to do for a living.
I paid more attention in school and I went on to graduate from Montana State University with degrees in mathematics. From there, being a high school math teacher and basketball coach was the path of least resistance. But the standard line is you can only teach Algebra II/Trig so many years in a row before the thrill is gone. From there, I went to the University of Washington in Seattle to work on my Ph.D. in statistics.
Q: That brings to me to one of my favorite anecdotes about you. You went to Seattle for your Ph.D., and during the first year of the program, your wife had your firstborn. By the third year, you had your second—at which point, you said, you got very "revenue-motivated."
Hereford: Yes, by the time our second kid rolled around I was indeed very revenue-motivated. Because what you get as a graduate research assistant at the University of Washington isn't really a living wage when you have two kids.
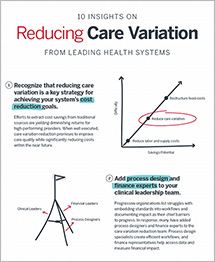
Get the Finance Leader's Resource Guide
But the move to health care was sheer coincidence. The department secretary sent a note around that Boeing was starting their 777 build. They were implementing TQM, and they needed somebody with platform skills to teach SPC and DOE. I didn't know what any of that meant, but I got to the next paragraph and it said, "We're paying $50 an hour contractor's wages"—and I very much knew what that meant. So I started teaching and then started doing some project work at Boeing. I then got involved in consulting with suppliers to Boeing and other companies on TQM.
While I was there, one of my clients was Group Health. That was one of the biggest pivots in my career, because it made me fall in love with health care—especially the mission-oriented people. Group Health ended up offering me a job, and I thought, "Well, this will be fun for a couple years and then I'll get back to my dissertation." Twenty years later, I was still there, having had a chance to learn from the variety of roles I played in a very innovative care organization.
Q: So you started at Group Health, then pivoted to Sutter's largest medical group, Palo Alto Medical Foundation (PAMF), and ended up at Stanford Health before taking on your latest role. Talk a little about that career progression.

Hereford: I had reached a good pivot point in my career at Group Health. My youngest had graduated from high school, and I knew at that point that I was either going to stay at Group Health my entire life or make a change professionally. And staying felt uncomfortable, you know? With every situation, I was beginning to go, "Oh, I know this situation. This is like the other three situations that we saw just like this." I was really starting to get hungry for new learning, new challenges.
PAMF happened to be recruiting for a COO, and they were very interested in pursuing ideas of Lean and Lean management—ideas I had brought to Group Health. I had had 20 years of experience in a very integrated organization, so I wanted to know what the great unwashed fee-for-service system looked like. It was just the right time.
I was at PAMF for about 18 months, during which we did a very rapid transformation, and I'm happy to say they are still going strong. Then I got a call from my buddy at Stanford Health. It was a difficult decision to leave PAMF after such as short time, but I don't regret it for a second in terms of what I was able to learn at Stanford over the last 4 years or so.
Lean philosophy and approach
Q: I understand, James, you're a big evangelist for Lean management techniques in health care. You have spoken in the past about our current, broken system that expects physicians to be 'heroic' and make a 'non-system' work—instead of just eliminating all the rampant inefficiencies. Say more about that.
Hereford: Your characterization is spot on. We've got a health care system right now that requires people to do heroic things to accomplish relatively straightforward things—we've overburdened providers with activities that have nothing to do with care delivery.
That's where Lean comes in, because this dysfunction as health care evolves into larger, more complex systems comes down to how we operate our systems and processes. That ability to really understand and manage your processes well is not what we do well in health care, despite the fact that we have a vast number of reports on how unsafe, low quality, and unreliable the care processes are.
Q: When you've spoken about Lean in the past, you've mentioned Autoliv—a Swedish airbag manufacturer in Ogden, Utah—that you'd like to take a delegation from Fairview to visit. What stuck with me was when you ask any Autoliv employee what they do, the answer is—
Hereford: "We save lives." It's not something that management told them to say when a visitor shows up, either. They believe it.
And yes, I'd like to take the board and senior management to visit Autoliv just so we have a sense of what great looks like. Between the time they started in the late 1990s and about 2013, Autoliv had a 17-fold increase in productivity simply by getting a little bit better constantly. They are nowhere close to a port, nowhere near Detroit, nowhere near an auto manufacturer of any sort—but they are a tier-one supplier for every car manufacturer in the world.Now, making airbags is different than health care delivery systems. But that attention to detail and the engagement of the staff—it's all driven by that ingrained belief in each employee that he or she is saving lives. What they do is straight forward, very machine and human-based, but incredibly disciplined, incredibly consistent, and the entire workforce is engaged in the pursuing excellence, and the results show in everything they do.
Coming to Fairview
Q: Let's pivot to Fairview. Before you assumed the CEO position, it was arguably the most scrutinized CEO vacancy in the nation, just because of how protracted the search was. I believe your hire took place almost 19 months after the prior CEO, Rulon Stacey, stepped down. And Fairview has had a turbulent recent history: for comparison's sake, Geisinger has had seven CEOs over a century—Fairview, five CEOs in five years.
Hereford: Yes that is very true. A complicated and definitely extended process. When I was approached with the role, I didn't know much about Fairview. I had heard a little bit here and there, but they weren't in the conversations that I was having around the best care delivery organizations in the country: the Intermountains, the Kaisers, etc.
But the more I read, the more intrigued I became. It felt like this organization was an incredibly undervalued asset, and that its primary problem was a lack of integration. I felt—and the board agreed—that the organization needed to move from a holding company to an operating company. Now, if I think of anything that has been consistent across the places I've been, it has been this idea of, "How do we integrate more effectively?" I loved that challenge.
I met with the selection committee, and I told them early on, "I'm not interested unless your aspiration is truly to be one of the best care delivery systems in the country. You have every potential, every attribute that you would want to have—it's just a matter of putting it together."
Of course, when I announced I was leaving Palo Alto to move to Minneapolis in December, you can imagine I got some interesting looks. But I said, "Well, look, it's like being told you have a Ferrari. And you go out, you open up the garage door, and sure enough there is a Ferrari there. It's just strewn in pieces across the floor—but if you put it together, you're going to have a heck of a car."
Q: You mention these pedigreed institutions—Intermountain, Kaiser, etc.—that enjoy a lengthy history and a clearly articulated identity. Just speculating, but I would think that one of the main advantages of Fairview is that after this period of transition you and your team can be instrumental in defining that identity anew.
Hereford: Yes, I agree with your thinking here. Fairview's in the position where it doesn't have to pull the kind of legacy structure with it like many other integrated care organizations. We've been good, but not yet great, and that means there's no success story we've got to overcome to enact change.
It's the sigmoid curve. You accelerate at some point and then at some point it starts to level off. And the challenge of organizations is figuring out how to jump from one sigmoid curve to the next one. For those other organizations, it's hard to be the interrupter of your own success, to really make that jump from one curve to another. So there's an opportunity for Fairview, if we're willing to seize it, to really think about our future, and what it's going to take to be an incredibly strong, capable care delivery system providing unique value to our community and to the state.
Market strategy
Q: There's a lot going on for Fairview these days. You've engineered the HealthEast merger (adding 3 hospitals and 14 clinics), you've incorporated the PreferredOne health plan into the health system, and you continue to iterate on the alignment structure with the University of Minnesota Physicians. How are you thinking about navigating these strategic issues, both a mixture of new and already 'in-flight' priorities?
Hereford: There's definitely no shortage of things to do. There was a lot of, "Well, let's wait for the new CEO," and so there is a certain amount of pent-up inventory. The dam burst a little bit when I started in December, but with that comes the opportunity to fundamentally think, and rethink, who we are and where we're going.
During those first few months, we took the senior team through a strategic refresh and just talked about who we are, what we're good at, and where we need to go. That was very helpful in getting a level of focus that I think is one of the most important attributes for any organization—we're not trying to chase all the shiny stars; we're focusing on the three or four things that you feel, "We've got to do this well."
Q: Let's dive more deeply into just one of these—prior to your arrival, Fairview exercised the option to purchase the additional 50 percent equity position in PreferredOne. That's about 185,000 lives altogether, of which about 50,000 or so are under full capitation. How are you thinking about a provider-sponsored health plan as a strategic asset in the context of some of the clinical and delivery system innovations you are implementing?
Hereford: Our health plan is never going to be a mega health plan. That is not our path or destiny. So within the state, I think we'll always be a contributor—but we're never going to be the answer.
But I am happy that we have a health plan for a few reasons. One, we get an opportunity to be innovative about bringing together both sides of the care continuum: the health plan and a care delivery system. Second, I think it's important to have some diversification in your revenue streams.
We have a large ASO business, and a network rental business, and I think that's very helpful, because developing good direct-to-employer relationships is part of what Fairview's challenge is, especially with medium and large employers. PreferredOne really gives us a more complete portfolio in terms of value-added possibilities—such as wellness programs or health analyses—for those medium and large employers. And I think that's important, because if you don't have that kind of a relationship you're simply a member of a network.
Q; The CEOs of some of the more tenured provider-sponsored health plans—Geisinger, Intermountain, Presbyterian—talk about creating a culture of a singular system with the delivery side and insurance side fully integrated. But what I heard you just describe, James, is different. It sounds as if you are intending to employ the health plan as an 'incubator' for delivery system innovation. Fair characterization?
Hereford: Yes, absolutely. I don't need to tell you how brutal the insurance game can be, certainly from an actuarial perspective. I think health plans are great at managing actuarial risk—that's what they do really well—but they're not great at managing care delivery risk. That is where care delivery systems have to be able to step up, and I'm not sure that care delivery systems, universally, have stepped up. There are certainly great examples: Group Health, Kaiser, Intermountain.
But I think the opportunity for Fairview is really to be able to think about, "What do we have to do from a care delivery system at both ends of the complexity spectrum?" Whether that's keeping healthy people healthy or figuring out the best way to manage people who are significantly sick. That ability for a care delivery system to manage care risk is critical.
Q: Let's turn to another key strategic priority for Fairview—your academic partnership and affiliation with the University of Minnesota. As I understand it, there are two different agreements?
Hereford: Yes. There's the 30-year affiliation agreement that was conceived of in 1997 and runs through 2027, and then we have the five-year MHealth agreement that was made in 2013. We're coming up on the opportunity to rethink that MHealth agreement, but we still have the long-term affiliation agreement.
Create a 21st century partnership strategy
Join us Oct. 25 to learn how to overcome obstacles that hinder successful partnerships
The opportunity here is huge. We have to be more than just competitive in the complex care, tertiary, quaternary space. We've got a very formidable competitor to the south of us—Mayo Clinic, you may have heard of them—but we can't take the backseat just because Mayo has this terrific track record of success. As we think about where the science of care is going, the University of Minnesota has a terrific set of platform skills such as genomics and computational science—a lot of things that are going to be absolutely essential as think about where care is going in the future.
I think academics are fundamentally rethinking what it's going to take to be successful in the future. But what got a Stanford, or a Penn, or a Hopkins into the position that they're in is not going to predict academic needs to be a top-20 going into the future. So I think that's our primary challenge in our relationship with the University of Minnesota: How do you leverage the value of academic care into a broad platform while maintaining permeable membranes that enable us to continue partnering strategically?
Q: How much of an impediment is it that you don't have a full-asset merger with the academic group?
Hereford: I think there are ways of conceiving of the relationship that don't require a full asset merger, that don't confuse or make oppositional the aspirations of being the best academic organization and the best community organization. The system we have to create has to be open to both of those aspirations.
We have to start with how to define ourselves, because right now we don't even have a word to describe who we are or what our relationship is, and that means we can't describe the value of it to the market. So we have to articulate what the relationship is, what it means to be together, and how I can support all of that. It's all about how best to organize ourselves to be as nimble, capable, and innovative as we need to be to meet the challenges that we have to meet.
Specialty pharmacy
Q: Escalating specialty pharmacy cost is one of the most contentious topics in the provider space, and of course only becoming more so. And now we're on to CAR-T and $475,000 gene-altering therapies, which will only enflame the issue further. But as you've characterized it, Fairview has one of the best specialty pharmacies out there with the Excelera Specialty Pharmacy Network. What did you discover that Fairview is doing uniquely?
Hereford: The ability to look into the near future and anticipate both the introduction of new drugs and then the management of existing treatments is key. So the authorization process is often a non-trivial task, as is ensuring that you're using the right drugs for the right reasons.
So if, as is often the case, there is a marginal benefit for a new treatment, it's making sure that people are aware of the alternatives that might be much more cost-effective and offer similar, or even the same, efficacy. And it's also scale: Are you procuring the drugs at a cost that gives you some advantage? We're at the size now with our specialty pharmacy that we get very advantaged discounting. We're not Kaiser, but the fact that we are as big as we are gives us a lot of leverage in the market. It's something we wouldn't necessarily have if it was just Fairview as a care delivery system standing on its own trying to acquire these drugs.
Q: I'm curious as to how you've actually inflected the cost curve here on what is now 15% of the health care dollar. From an outside perspective, everything you're doing on the adherence front, medication reconciliation, embedding pharmacists into the care management team, etc. All that seems progressive but not revolutionary. What's the secret ingredient?
Hereford: The impact is difficult to tease out with exactness, but the impact is definitely there. We realize significant benefit in our overall budget. It's always hard to prove the counterfactual—what would it have been if you didn't have this capability—but we certainly are managing that part of cost line much more effectively than I have in previous organizations where you're more exposed to the market price.
The thing I love about our specialty pharmacy is it's also doing a great job of owning the complexity for patients, because that's often who gets caught in the middle of all this. At a different organization, a physician might recommend a medication, and the patient realizes it's too expensive, and then the patient is caught in this loop of, "Well, you've got to go back to your physician." In our specialty pharmacy, the specialty pharmacist program is able to step into the middle of that and really simplify the process a great deal.
Final thoughts
Q: As we finish up, James, I'd like to do a final reflection on your career progression. You've traversed so many parts of the health care ecosystem—from the payer side to the physician side to the complex academic system side, really, pretty much everything but the public policy and governmental side—
Hereford: —which I'm hoping to be able to continue to avoid if I can.
Q: A wise man. Now on the one hand, you might characterize your background—from teaching mathematics and coaching basketball all the way to your current work—as non-linear. But from a retrospective point of view, you might well have the perfect background to do the transformational work you're trying to do at Fairview. In the moment, though, did it feel more serendipitous than intentional?
Hereford: Great question. I actually think it is both. Probably a combination of being an aggressive learner and damn lucky. When grad students ask me for career advice, I keep telling them, "Look, just get involved in the hardest projects you can. Any organization you go into, find the hard project, be a part of it. It'll give you more visibility, because you'll be seen by more people in the organization."
But, you know, I was also just fortunate. A lot of really interesting problems came my way, and then I was pretty aggressive about learning about medicine. When I was at that perfect ecosystem of Group Health, from a rational care delivery perspective, I didn't really know what an academic inpatient environment was like—so where else to go learn but at Stanford?
I think the fact that I can sit here now and say, "Well, yeah, I've had some good experiences that I can bring to bear at Fairview"—that's probably more luck than anything. But it's also the active acquisition of new experiences, right? New learning, new things to explore.
Get more lessons from the C-suite
Check out our recent must-read interviews with other top hospital and health system leaders:
 From India to Urban America: How Ram Raju's experience serving underserved communities is redefining patient-centered care at Northwell Health
From India to Urban America: How Ram Raju's experience serving underserved communities is redefining patient-centered care at Northwell Health
Ram Raju, SVP and Community Investment Officer at Northwell Health, talks about the "art and science" of addressing social determinants of health, a career sparked by his father's experience following Gandhi's fight for India's independence, and why we need to move from provider-based outcomes to patient-based outcomes. Read our interview with Ram.
 Can two CEOs co-lead? Bob Garrett and John Lloyd are showing how it's done.
Can two CEOs co-lead? Bob Garrett and John Lloyd are showing how it's done.
Bob Garrett and John Lloyd, co-CEOs of Hackensack Meridian, talk about their unique leadership structure, building a medical school for tomorrow's doctors, and what will headline Hackensack Meridian's press releases for 2022. Read our interview with Bob and John.
 As a soldier, Legacy's CEO witnessed the fall of the Berlin Wall. Here's how George Brown is serving his system now.
As a soldier, Legacy's CEO witnessed the fall of the Berlin Wall. Here's how George Brown is serving his system now.
George Brown, CEO of Legacy Health System, talks about transitioning into civilian care after years in the military, addressing the social determinants of health, and collaborating with non-traditional partners. Read our interview with George.
Don't miss out on the latest Advisory Board insights
Create your free account to access 1 resource, including the latest research and webinars.
Want access without creating an account?
You have 1 free members-only resource remaining this month.
1 free members-only resources remaining
1 free members-only resources remaining
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
You've reached your limit of free insights
Become a member to access all of Advisory Board's resources, events, and experts
Never miss out on the latest innovative health care content tailored to you.
Benefits include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This content is available through your Curated Research partnership with Advisory Board. Click on ‘view this resource’ to read the full piece
Email ask@advisory.com to learn more
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox
This is for members only. Learn more.
Click on ‘Become a Member’ to learn about the benefits of a Full-Access partnership with Advisory Board
Never miss out on the latest innovative health care content tailored to you.
Benefits Include:
Unlimited access to research and resources
Member-only access to events and trainings
Expert-led consultation and facilitation
The latest content delivered to your inbox